BURSAE
Anatomy:
- Bursae are fluid-filled sacs located near tendons,
ligaments,
skin,
and muscles that prevent friction between moving structures.
- There are multiple bursae located at the base of the metatarsals and between the metatarsal bones in the intermetatarsal spaces located in the forefoot.
Intermetatarsal Bursitis (IMB)
- Inflammation of the intermetarsal bursae (bursitis) can occur following trauma or secondary to systemic diseases such as rheumatoid arthritis,
gout or local irritation (Morton's neuroma).
- Severe bursitis results in distension of the bursa causing fore foot pain and splaying of the digits either side of the intermetatarsal space (‘daylight sign’).
(13)
MRI Features:
- The single most distinguishing feature of a IMB is its location - at pressure points between the metatarsal joints.
- Well-defined fluid collection demonstrating T1-hypointensity and corresponding T2 and STIR hyperintensity.
- Peripheral enhancement is seen following contrast administration.
- Size of the bursa is an important factor in diagnosing bursitis (14).
Learning point: Small fluid collections with a transverse diameter of less than 3 mm in the first three intermetatarsal bursae are usually physiologic
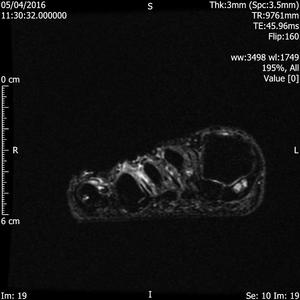
Fig. 1: Intermetatarsal bursitis of 3rd space: STIR axial image of forefoot shows hyper intense fluid signal in 3rd intermatatarsal space with mild medial sesamoiditis:
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
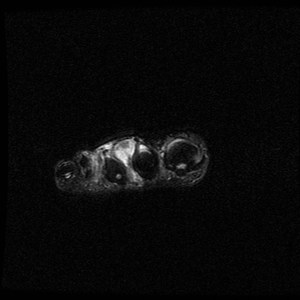
Fig. 2: Intermetatarsal bursitis: STIR axial image of forefoot shows hyper intense fluid signal in 2rd intermatatarsal space .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
MORTONS NEUROMA
- Morton's Neuroma (MN) is an interdigital mass thought to arise secondary to compression and ischaemia of neural tissue.
The mass is composed of perineural fibrotic tissue and is most commonly found between the 3rd and 4th metatarsal heads.
(7)
- Common incidental finding in the middle-aged population -majority of patients are asymptomatic with upto 30% of middle-aged people thought to have radiologic findings of a MN.
- Female predominance - high heeled shoes have been implicated as a cause.
- Symptomatic patients present with pain at the metatarsal heads -classically radiates from the mid-foot to the toes and worsens with activity.
(8)
MRI Features:
- Best detected in the coronal plane.
- Variety of sequences described in the literature - including T1-weighted inversion recovery ,
T1-weighted fatsuppressed images with gadolinium enhancement and also T2-weighted (9).
- In our centre we have found the use of T1-weighted sequences particularly useful.
Learning point: Detection of Morton's Neuroma with MRI only becomes relevant when the transverse diameter of the lesion measures 5 mm and the lesion can be correlated with the clinical findings.(9)
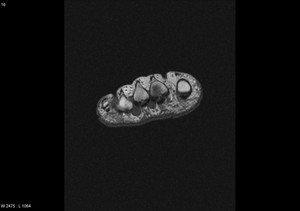
Fig. 3: Morton's neuroma: T1 axial image of forefoot shows well defined intermediate signal intesity lesion Morton's neuromas in 2nd and 3rd intermaetatarsal spaces.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK

Fig. 4: Morton's neuroma: Large Morton's neuroma in 3rd intermatatarsal space of forefoot.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
DEGENRATIVE JOINT DISEASE
1) Osteochondral lesion of 1st metatarsal head
- Osteochondritis dissecans (OD) is a form of traumatic arthritis.
- Within the forefoot OD commonly affects the first metatarsal head.
The disease represents an unhealed osteochondral defect,
which progresses to degenerative arthritis if left untreated.
- The familiar OD staging system can be applied to the OD of the 1st MTH with stage 4 indicating a displaced intra-articular fragment.
- MRI is vital in detecting the separation of the osteochondral fragment.
MRI Features:
- T1-weighted images show low signal adjacent to the fragment.
Corresponding T2-weighted images demnonstrate a hyperintense line demarcating a,
usually hypointense,
fragment.
The donor site can also be identified as high signal area (2).

Fig. 5: Osteochondral lesion of 1st metatarsal head: T1 coronal image of forefoot shows osteochondral lesion of 1st metatarsal head in subarticular distribution.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK

Fig. 6: Metatarsal-sesamoid joint OA :T2 Fat sat sagittal image of hallux shows chondropathy at Metatarsal-sesamoid with subchondral bright signal intensity .There is also mild subjacent synovitis and effusion.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
2) Freibergs Disease
- Freibergs Infraction/ Disease is a relatively uncommon but well recognised osteochondrosis of the metatarsal heads first described in 1914 by Albert Freiberg (10).
- Thought to occur secondary to acute or repetitive injury and vascular compromise.
- Generally affects adolescent women (high heeled shoes are a risk factor) who present with pain and a restricted range of motion.
- First symptoms often manifest themselves when degenerative arthritis has already developed.
- Typically affects the 2nd and 3rd metatarsal heads and can be bilateral in up to 10%.
(2)
MRI Features
- Early findings include hypointense signal in the metatarsal heads on T1-weighted images with hyperintensity on T2-weighted and STIR images.
- With disease progression hypo-intense change develops on T2-weighted images as the bone becomes sclerotic .
Learning point: Architectural changes resulting in flattening of the metatarsal heads is a characteristic late finding (2).
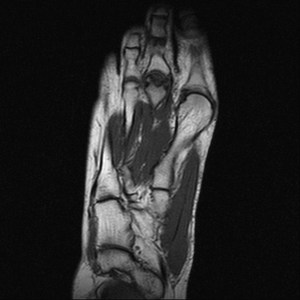
Fig. 7: Freiberg disease:T1 coronal and sagittal MRI image of forefoot shows flattening of the second metatarsal head with low-signal-intensity changes in the second metatarsal head .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
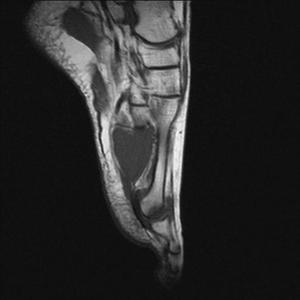
Fig. 8: Freiberg disease:T1 coronal and sagittal MRI image of forefoot shows flattening of the second metatarsal head with low-signal-intensity changes in the second metatarsal head .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
SESAMOIDS
Anatomy
- Sesamoids are pea-sized bones embedded on the plantar aspect of the foot.
They are found at the medial (tibial) and lateral (fibular) aspect.
Sesamoiditis
- Sesamoiditis is a form of tendinitis induced by repetitive injury to the plantar surface of the forefoot typically affecting young athletes (12).
MRI Features
- Bone marrow of the sesamoid bones demonstrate hyperinstensity on STIR images and hypointensity on T1-weighted imaging.
- These intensity changes are similar to those seen in stress response.
- Involvement of both sesamoid bones favours a diagnosis of sesamoiditis.
- Other characteristic findings include reactive soft-tissue changes,
including tendinitis,
synovitis,
and bursitis (2).
Learning point: If the signal intensity of the bone marrow in the sesamoid bones is hyperintense on STIR images but normal on T1-weighted images,
a diagnosis of sesamoiditis is favourable to stress response.
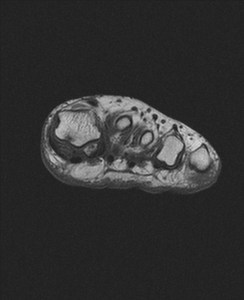
Fig. 9: Medial sesamoiditis: T1 axial and coronal images of forefoot show biparite medial sesamoid bone with low signal intensity within the bone.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK

Fig. 10: Medial sesamoiditis: T1 axial and coronal images of forefoot show biparite medial sesamoid bone with low signal intensity within the bone.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
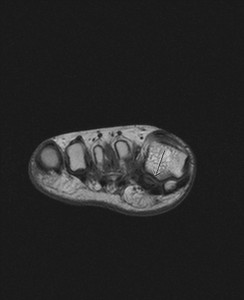
Fig. 11: Lateral sesamoiditis :T1 axial images of forefoot show low signal intensity within the lateral sesamoid bone.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
TRAUMA -Soft Tissue
Turf toe
- Traumatic hyperextension injury of the toe resulting in plantar plate injury.
- Usually affects athletes playing on artificial surfaces.
- Injury ranges from sprain to complete tear of the plantar plate- fibrocartilaginous complex resulting in unrestricted range of motion (ROM) of the 1st MTP joint.
(12).
MRI features vary according to grading:
- Key features include plantar plate involvement with hyperintensity seen plantar to the sesamoid bones on STIR and T2-weighted images.
- Complete rupture manifests as a discontinuity in the in the plantar plate along with increased signal intensity in the soft tissues (2).
- Articular cartilage and subchondral bone injury can also be assessed for grading (2).
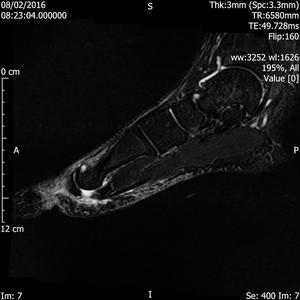
Fig. 12: Turf toe: T2 fat suppressed sagittal and axial images of forefoot show rupture of plantar plate of 1st MTP joint.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
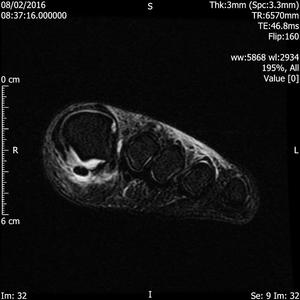
Fig. 13: Turf toe: T2 fat suppressed sagittal and axial images of forefoot show rupture of plantar plate of 1st MTP joint.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
TRAUMA- Osseous
1) Metatarsal Stress Response
- Stress-response in the fore foot has a non-specific presentation following repetitive injury to the metatarsals.
- There is often a history of overuse and diagnosis is vital in preventing the sequela of a stress fracture.
MRI Features
- Indistinct area of hypo-intense bone marrow on T1-weighted images with corresponding T2 and STIR hyperintensity .
- Oedema is usually present in the adjacent soft tissues,
and there is enhancement following contrast administration (2).
Learning point: A stress response can progress to a stress fracture,
which is characterised by a band of cortical hypointensity on both T1- and T2-weighted images.
2) Stress fractures
- Stress fractures (fatigue fractures) in the metatarsal bones occur due to a discrepancy between chronic mechanical stress placed on the bone and the strength of the bone.
- They are most common in athletes (runners) and in the foot they commonly affect the middle-to-distal shaft of the 2nd,
3rd and 4th metatarsal diaphyses.
- Stress injuries can also occur in the sesamoid bones of the hallux.
MRI features:
- Hypointense line (fracture) extending through the cortex and into the medullary cavity on both T1- and T2-weighted images.
- STIR high signal in keeping with oedema in the surrounding marrow is common (2).
Learning point: Subchondral metatarsal fractures in diabetic patients with neuropathic arthropathy can appear identical to a stress fracture and thus clinical context is key to diagnosis.

Fig. 14: Metatarsal stress response: STIR axial image of forefoot shows bone marrow oedema and circumferential inflammatory changes around the 2nd metatarsal shaft.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
3) Fracture of proximal phalynx.
- Proximal phalanx fractures occult on Xray can be detected on MRI .
MRI Features:
- Fracture line extending through the cortex and into the medullary canal which is hypointense on both T1- and T2-weighted images.
- There is usually STIR high signal in keeping with oedema in the surrounding marrow.
Learning point: MRI is particularly useful in detecting occult fractures in osteopenic patients.
(2,
6)

Fig. 15: Fracture of proximal phalanx, plain radiograph was normal:T1 and T2 fat sat sagittal images of forefoot show corner fracture in base of proximal phalanx seen as low signal intensity line . There is associated bone marrow oedema seen as bright signal intensity on T2 fat sat images.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
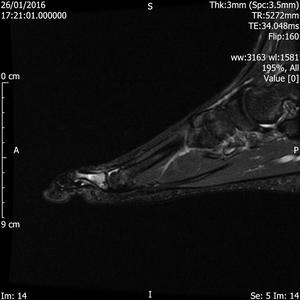
Fig. 16: Fracture of proximal phalanx, plain radiograph was normal:T1 and T2 fat sat sagittal images of forefoot show corner fracture in base of proximal phalanx seen as low signal intensity line . There is associated bone marrow oedema seen as bright signal intensity on T2 fat sat images.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
INFLAMMATORY TENDON ABNORMALITY
Anatomy
- The flexor tendon group is responsible for flexion of the toes and ankle.
- In the forefoot the main flexor tendons are the flexor hallucis longus; flexor hallucis brevis and flexor digitorum longus.
Tensoynovitis of flexor tendon
- Tenosynovitis is inflammation of the synovial membrane surrounding a tendon and usually occurs secondary to inflammatory conditions (RA,
Gout),
infection or local irritation.
- Symptoms include tenderness along the length of the tendon.
Pain may be in the arch of the foot,
on the inside of the ankle and pain on resisted flexion of the hallux.
- In the forefoot the flexor hallucis longus is subject to repetitive impact between the sesamoid bones and under the base of the 1st MT ,
where the flexor hallucis longus crosses over the flexor digitorum longus.
These are common sites of tenosynovitis (2,
5).
MRI features:
- Fluid accumulation is seen within the sheath.
- Characteristic post contrast enhancement of the sheath occurs.
- Chronic inflammation results in a stenosing tenosynovitis causing fibrosis and tendon entrapment.
- MR findings in stenosing tenosynovitis include thickening of the tendon or tendon sheath,
increased fluid within the tendon sheath,
and post contrast enhancement of the tendon sheath (2,4-5).
- Tendon degeneration and rupture are also potential late sequela.
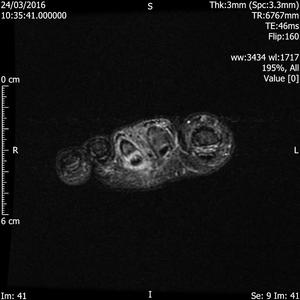
Fig. 17: Flexor tenosynovitis: STIR axial image of forefoot shows hyper intense fluid signal surrounding the flexor tendon leading to 3rd toe . The flexor tendon itself appears swollen on comparison to subjacent tendon and shows intrinsic bright signal and heterogeneity .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
SYNOVIUM
Anatomy:
- Synovial membrane lines the joint capsule producing synovial fluid (Pannus) which lubricates the joint.
- Inflammation of the joint capsule can be termed synovitis or capsulitis. Synovitis results in increased production of synovial fluid causing swelling of the joint.
Inflammatory arthropathy -Synovitis of MTP joints
- Rheumatoid arthritis commonly affects the feet with early changes at the MTP joints (2,
5).
MRI Features:
- Pannus demonstrates low to intermediate signal intensity on T1-weighted.
Signal intensity may vary on T2-weighted images.
- T2 hyperintensity indicates hypervascular pannus.
- As disease progresses a fibrous pannus develops and hemosiderin deposition may occur,
demonstrating low signal intensity on T2-weighted images.
- MR imaging can also be used to better depict complications such as ruptures of the ligaments and tendons,
bursitis,
and loss of articular cartilage.
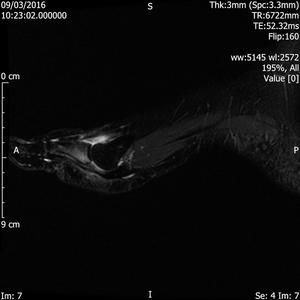
Fig. 18: Synovitis of 1st MTP joint: STIR sagittal image shows joint effusion and synovitis of 1st MTP joint.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
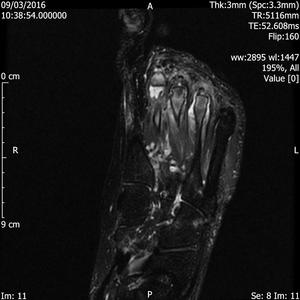
Fig. 19: Synovitis of MTP joints: STIR coronal and axial images of forefoot show joint effusion , synovitis and subarticlar bone marrow oedema of 2nd, 3rd and 4th MTP joints in a patient with known inflammatory arthropathy.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
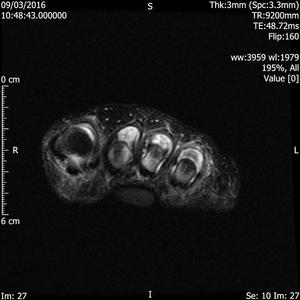
Fig. 20: Synovitis of MTP joints: STIR coronal and axial images of forefoot show joint effusion , synovitis and subarticlar bone marrow oedema of 2nd, 3rd and 4th MTP joints in a patient with known inflammatory arthropathy.
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
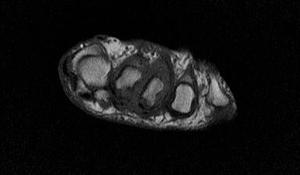
Fig. 21: Inflammatory synovitis: T1 axial images of forefoot show intermediate signal intensity thickened synovial rind of 2nd, 3rd MTP joints .There is also a small erosion at 2nd metatarsal head .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK
NEOPLASTIC LESIONS
Fibroadenoma
- Nodule or mass in the medial aspect of the plantar surface which can extend into the deep structures of the foot.
- Lesions can cause mass effect or invasion of adjacent muscle or neurovascular structures.
- Plantar fibromatosis can be seen in both children and in adults with a male predilection.
MRI Features
- Lesions have low to intermediate signal on T1-weighted MR images and usually low signal intensity on T2-weighted images.
- Contrast enhancement is variable.
(15)
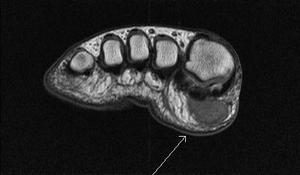
Fig. 22: Fibroadenoma of foot :T1 sagittal and axial MRI images of forefoot show a well defined intermediate to low signal intensity lesion in the subcutaneous fat pad of ball of hallux .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK

Fig. 23: Fibroadenoma of foot :T1 sagittal and axial MRI images of forefoot show a well defined intermediate to low signal intensity lesion in the subcutaneous fat pad of ball of hallux .
References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK























