ESSR 2016 / P-0059
Ultrasound evaluation of knee trauma
Congress:
ESSR 2016
Poster Number:
P-0059
Type:
Educational Poster
Keywords:
Athletic injuries, Trauma, Education, Diagnostic procedure, Ultrasound, Musculoskeletal soft tissue, Musculoskeletal joint, Musculoskeletal bone
Authors:
S. P. Ivanoski1, B. Tolovski2, V. Vasilevska Nikodinovska2; 1Ohrid/MK, 2Skopje/MK
DOI:
10.1594/essr2016/P-0059

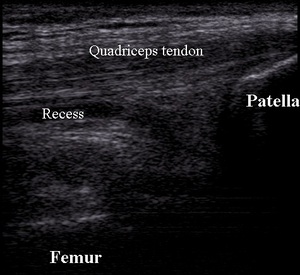
Fig. 1:
Normal quadriceps tendon and suprapatellar recess

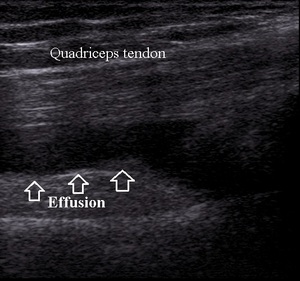
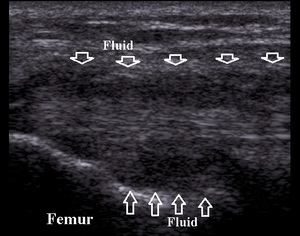
Fig. 2:
Moderate effusion in suprapatellar recess

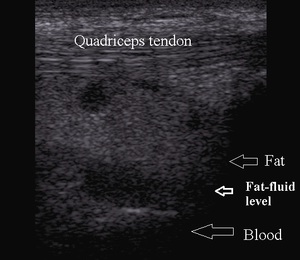
Fig. 3:
Suprapatellar recess lipohemarthrosis

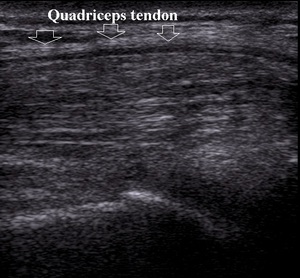
Fig. 4:
Quadriceps tendon tendinitis

Fig. 5:
Normal patellar ligament

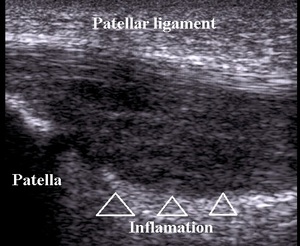
Fig. 6:
Patellar ligament inflamation

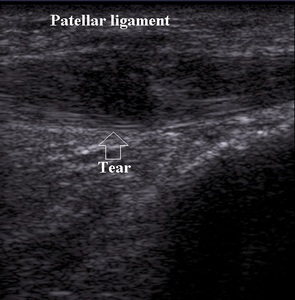
Fig. 7:
Partial thickness tear of patellar ligament

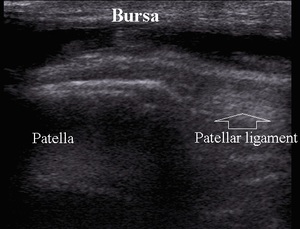
Fig. 8:
Prepatellar bursitis

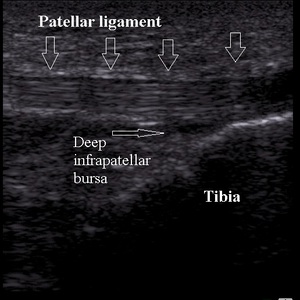
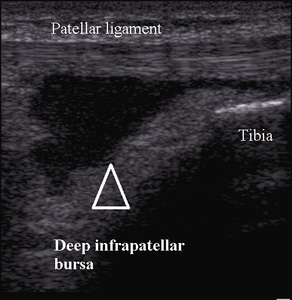
Fig. 9:
Deep infrapatellar bursitis

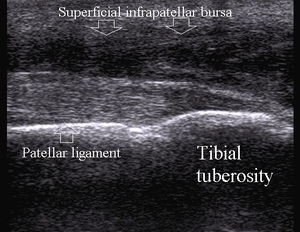
Fig. 10:
Superficial infrapatellar bursitis

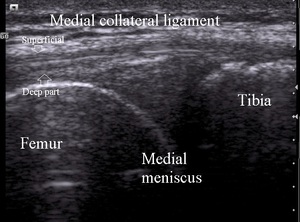
Fig. 11:
Medial knee normal anatomy

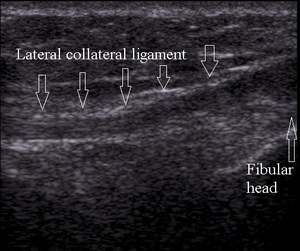
Fig. 12:
Normal lateral collateral ligament

Fig. 13:
Lateral collateral ligament partial thickness tear

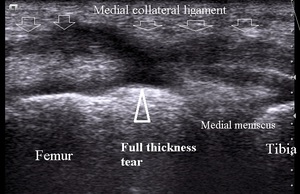
Fig. 14:
Medial collateral ligament full thickness tear

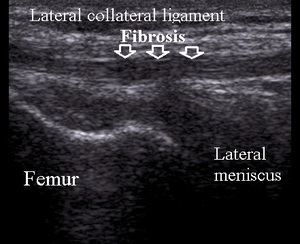
Fig. 15:
Lateral collateral ligament chronic tear

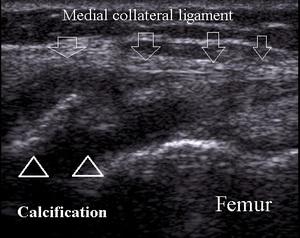
Fig. 16:
Pellegrini-Stieda lesion

Fig. 17:
Lateral knee normal anatomy

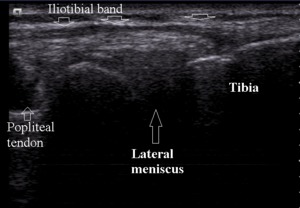
Fig. 18:
Normal iliotibial band

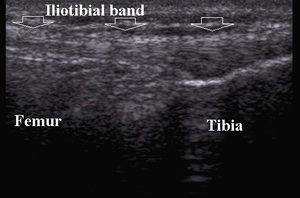
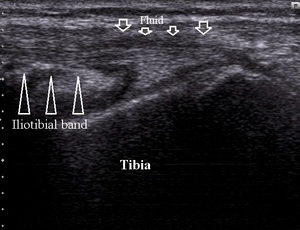
Fig. 19:
Iliotibial band friction syndrome

Fig. 20:
Segond avulsion fracture

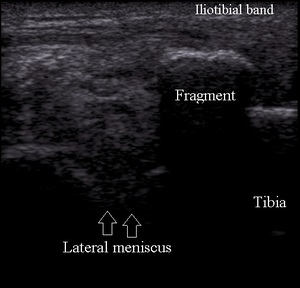
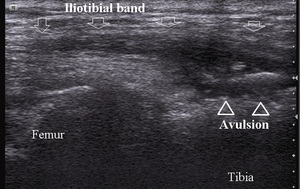
Fig. 21:
Iliotibial band avulsion fracture

Fig. 22:
Normal medial patellar retinaculum

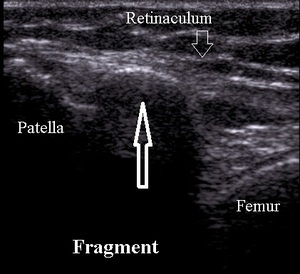
Fig. 23:
Medial patellar facet osteochondral fracture

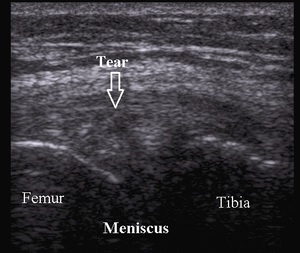
Fig. 24:
Medial meniscus tear

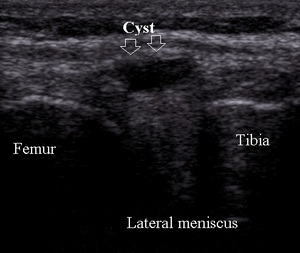
Fig. 25:
Lateral meniscal small cyst