ESSR 2016 / P-0097
Fat pillows of the knee, not always so soft!
Congress:
ESSR 2016
Poster Number:
P-0097
Type:
Educational Poster
Keywords:
Musculoskeletal soft tissue, Anatomy, MR, Education, Pathology
Authors:
A. C. Vieira, A. Vieira, R. Cunha; Porto/PT
DOI:
10.1594/essr2016/P-0097

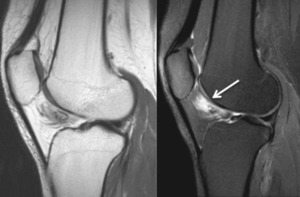
Fig. 3:
Sagittal PD fat sat; Anterior suprapatellar impingement syndrome

Fig. 4:
Sagittal T2 fat sat; Anterior suprapatellar impingement syndrome

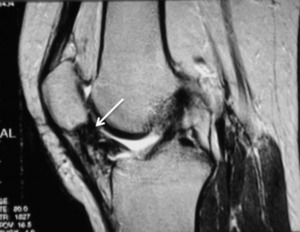
Fig. 5:
Sagittal T2 fat sat; Hoffa disease

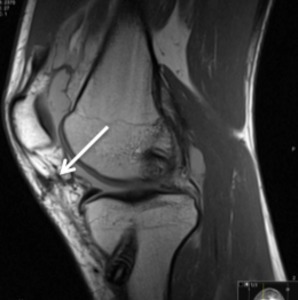
Fig. 6:
Sagittal PD fat sat; Impingement of the superolateral aspect of the...

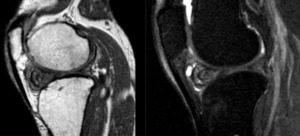
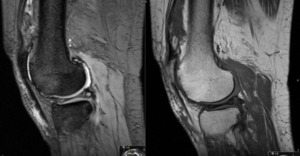
Fig. 7:
Sagittal T1 fse and T2 fat sat; Infrapatellar plica syndrome

Fig. 8:
Sagittal T2 fat sat; Posterior suprapatellar fat pad impingement in a patient...

Fig. 9:
Sagittal T2 fat sat; Edema of the anterior and part of the posterior...

Fig. 10:
Sagittal T2 FSE; Arthrofibrosis

Fig. 11:
Sagittal PD; Linear fibrosis post-arthrocopy

Fig. 12:
Sagittal T1 and T2 fat sat; Cyclops lesion in a patient with ACL reconstruction

Fig. 13:
Sagittal T1; Deep infrapatellar bursitis
")
Fig. 14:
Sagittal PD fat sat; Ganglionic cyst (no meniscal tear)

Fig. 15:
Sagittal T2 * and T1 SE; Suprapatellar villonodular synovitis

Fig. 16:
Sagittal T2 FSE - Infrapatellar villonodular synovitis