ESSR 2017 / P-0169
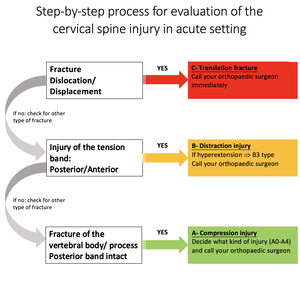
Cervical spine trauma: When best to call your orthopedic spine surgeon immediately. Understanding classification systems.
Congress:
ESSR 2017
Poster Number:
P-0169
Type:
Educational Poster
Keywords:
Trauma, Education and training, Acute, Surgery, Structured reporting, Education, MR, CT, Musculoskeletal spine, Musculoskeletal joint, Musculoskeletal bone
Authors:
M. Kaniewska1, A. Mameghani1, T. Specht1, M. P. Pelczar2, R. A. Kubik-Huch1, S. E. Anderson1; 1Baden/CH, 2Nottwil/CH
DOI:
10.1594/essr2017/P-0169

Fig. 10:
ACR Appropriateness Criteria for imaging when acute cervical spina trauma is...

Fig. 11:
ACR Appropriateness Criteria for imaging when acute cervical spina trauma is...

Fig. 12:
ACR Appropriateness Criteria for imaging when cervical spine is unstable and...

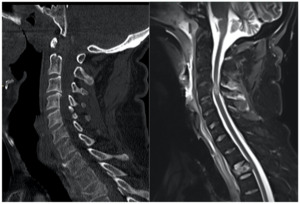
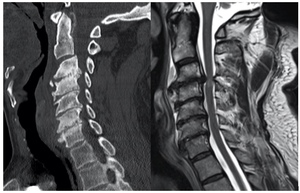
Fig. 13:
Sagittal CT reconstructions show a translation injury through C6/C7,...
 References: AOSpine")
Fig. 14:
Type A- Compression injuries with subtypes (A0-A4)
 References: AOSpine")
Fig. 15:
Type B- Distraction injuries with subtypes (B1- B3)

Fig. 16:
Type C- Translation injuries.
Only one fracture type.

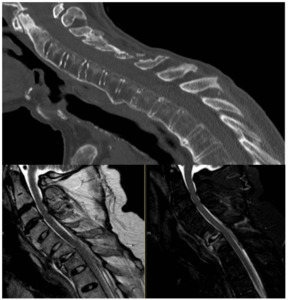
Fig. 17:
Type F- Additional type of fracture with injury of a facet joint.
 and a non-displaced fracture of the spinous process of C5 (classified separately as A0 fracture).
Note traumatic changes of soft tissues and ligamentous structures of the posterior column. C3-C6 cord hemorrhage is evident. References: Swiss Paraplegic Centre, Nottwil, Switzerland")
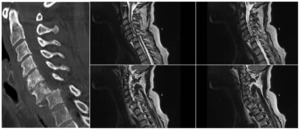
Fig. 22:
Sagittal CT and sagittal T2w MR exams show a hyperextension injury through C5/6...

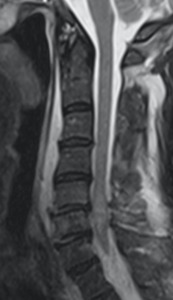
Fig. 23:
Sagittal T2w MRI presents a hyperextension injury through C6/7. Note traumatic...
. Traumatic disc herniation should be separately evaluated in the MRI.")
Fig. 25:
Translation injury with a subluxation through C5/6 and consecutive spinal cord...

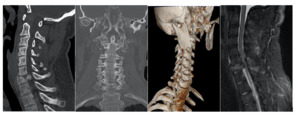
Fig. 26:
Sagittal and coronal CT show a translation injury through C5/6 with concomitant...

Fig. 27:
Sagittal CT, T2w MRI and axial T2w.
Cord transection with a complex...
.
Images from left to right:
1. Localisation of the fracture
2. Placement of distraction pins into C4 and C6
3. Corporectomy of fractured C5. Stabilisation with iliac crest graft and locking plate
4. Final image References: Swiss Paraplegic Centre, Nottwil, Switzerland")
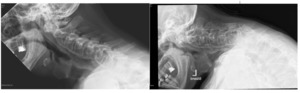
Fig. 28:
Intraoperative fluroscopic images of the surgical stabilisation of the fracture...

Fig. 29:
Sagittal CT and postoperative radiographs of the translation injury through...

Fig. 35:
Sagittal and axial CT examination show a gunshot injury with right-sided...

Fig. 36:
Sagittal CT and T2w FatSat MRI demonstrate a traumatic discoligamentous injury...

Fig. 37:
Sagittal T2w, T1w and axial T2w MRI show a burst fracture of C5 with spinal...

Fig. 38:
Sagittal T1w, T2w and STIR images show a traumatic disc herniation through...