
ESSR 2017 / P-0266
Sacral bone tumors
Congress:
ESSR 2017
Poster Number:
P-0266
Type:
Educational Poster
Keywords:
Musculoskeletal system, Musculoskeletal spine, Musculoskeletal bone, CT, MR, Conventional radiography, Diagnostic procedure, Cancer, Tissue characterisation
Authors:
B. Ruiz1, J. J. Gomez Muga1, F. Diez Renovales1, J. Cardenal Urdampilleta1, M. Sarmiento1, S. Delgado Saiz2; 1Bilbao/ES, 2Brakaldo /ES
DOI:
10.1594/essr2017/P-0266

Fig. 1:
Giant Cell Tumor. A 27 year old woman with cauda equina syndrome. Urgent MRI...
. CT coronal, sagital and axial images with bone and soft tissue window reveals a lytic solid tumor, located in midline, in the sacrum that produces posterior wall erosion and invasion of the spinal canal. On last images we can see CT- guided biopsy.")
Fig. 2:
Giant Cell Tumor (Same patient). CT coronal, sagital and axial images with...
. Angiography shows a very vascularized mass with arterial afferents from 5 pedicles: Both lateral sacral arteries, middle sacral artery and a distal branch of left internal iliac artery. The five arterial pedicles were embolized prior to surgery.")
Fig. 3:
Giant Cell Tumor (Same patient). Angiography shows a very vascularized mass...

Fig. 4:
Giant Cell Tumor. 47 year old patient who has had tumor resection twice and...

Fig. 5:
Benign notochordal cell tumour: A 50-year-old woman. In a lumbar MR study was...
. CT images show slight bone sclerosis without lytic areas or any other suspicious sign. Patient underwent biopsy in another center confirming the nature.")
Fig. 6:
Benign notochordal cell tumour: (same patient). CT images show slight bone...

Fig. 7:
Benign notochordal cell tumour: 61 year old woman. In a lumbar MR study was...

Fig. 8:
Benign notochordal cell tumour: 57 year old woman. In a lumbar MR study was...
 and S1 in patient B) which shows hyperintensitiy on both T1 and T2 –weighted images.")
Fig. 9:
Hemangioma: Two diferent patients showing as a casual finding in a lumbar MR...

Fig. 10:
Vascular proliferation with mild atypia. 57 years old man studied due to...
. A) Bone window CT images show lytic lesion. B) Soft tissue window contrast enhanced CT images show enhancing mass with expansive component located in S2 protruding into the canal. C) CT guided biopsy.")
Fig. 11:
Vascular proliferation with mild atypia. (Same patient). A) Bone window CT...
. 5 year interval exploration show progressive growth of the lesion.")
Fig. 12:
Vascular proliferation with mild atypia (same patient). 5 year interval...

Fig. 13:
Epithelioid hemangioendothelioma: 25 year old man with long standing low back...
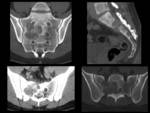
Fig. 14:
Epithelioid hemangioendothelioma (same patient): non enhanced CT show lytic...
: A) angiography demonstrate a very vascular mass. B) embolization of the lesion prior to resection.")
Fig. 15:
Epithelioid hemangioendothelioma (same patient): A) angiography demonstrate a...

A) Contrast-enhanced CT and B) MRI shows partial resection of the mass with remaining tumor at the level of S2 and extending to sacral alae.")
Fig. 16:
Epithelioid hemangioendothelioma (same patient 5 months later)
A)...
. MR imaging showing progressive growth of the mass.")
Fig. 17:
Epithelioid hemangioendothelioma (same patient 5 years later). MR imaging...

Fig. 18:
Chordoma: 41years old man. In lumbar MRI we can see lytic lobulated soft tissue...
 In lumbar CT we can see the lytic sacral changes with areas of sclerosis and the lobulated soft tissue mass extending to presacral space and sacral canal. Calcifications may be seen inside the mass. In the last image we can see hypo echogenic soft tissue mass in US, used to guide biopsy. References: department of radiology, Hospital Universitario Cruces")
Fig. 19:
Chordoma (same patient) In lumbar CT we can see the lytic sacral changes with...

Fig. 20:
Chordoma: 63 year old man who after trauma refers pain and sacral bulge. Non...
: MR imaging show sacrococcygeal tumor with bone infiltration. Polilobulated appearance of the soft tissue mass which is highly hyperintense on T2-weighted images, hypointense on T1 with mild enhancement in the inferior margin.")
Fig. 21:
Chordoma (same patient): MR imaging show sacrococcygeal tumor with bone...

Fig. 22:
Chordoma. 75 year all woman with partial resection of chordoma. Remains a...
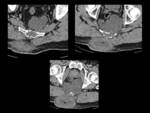
Fig. 23:
Chordoma. Same patient. Axial CT show same findings. Sacrococcygeal tumor with...
 CT that reveals a lytic lesion with soft tissue mass in left S1 B) MR demonstrate on the left side of the vertebral body of S1 which extends to the ipsilateral ala. It is highly hypointense on T1 weighted images, heterogeneous on t2, and after contrast administration there is a central solid uptake and peripheral hyperintensity/necrosis C) Growth of the mass after six months.")
Fig. 24:
Metastatic lymphoma: 81-year-old male with B-cell lymphoma. A) CT that reveals...

Fig. 25:
Metastatic lymphoma 74-year-old male with B-cell lymphoma under chemotherapist...

Fig. 26:
Metastatic disease. A 72-year-old woman under oncological CT control due to...
 On CT we can see a large lytic mass in the left hemisacral bone interrupting cortical extending through the spinal canal, foramina and sacroiliac joint. B) MRI show the highly hyperintense large sacral mass. C) CT guided biopsy. D) contrast enhance CT at the neck reveals a small nodule in right thyroid lobule and a mainly hypo attenuating enlargement of the left thyroidal lobe.")
Fig. 27:
Metastatic disease: A 72 year old woman. A) On CT we can see a large lytic mass...
: PET TC demonstrate FDG pathologic uptake in left thyroid lobe, left hemisacral bone and a cervical posterior arch metastasis.")
Fig. 28:
Metastatic disease (same patient): PET TC demonstrate FDG pathologic uptake in...
: thyroid US demonstrating a left lobe heterogeneous nodule and its biopsy which resulted to be a papillary carcinoma as the primary tumor.")
Fig. 29:
Metastatic disease (same patient): thyroid US demonstrating a left lobe...

Fig. 30:
Metastatic disease: 74 year old person. Lumbar spine X-ray, CT and MRI show a...
: multinodular goiter with suspicious nodule that resulted to be a papillary cancer.")
Fig. 31:
Metastatic disease (same patient): multinodular goiter with suspicious nodule...