All patients who underwent a CT study of the foot for a suspected/known acute trauma injury during a period of 3 years (January 2013 to December 2016 inclusive) at our Hospital were identified by inspecting the digital database of our Picture Archiving and Communication ystem.
Over the stated period,
33 had evidence of a calcaneal fracture.
Of these,
illustrative cases were selected to discuss the value of multidetector CT and the use of Sanders and Regazzoni classification systems for the evaluation of calcaneal fractures.
Type of fractures
Fractures of the calcaneus are divided into intra-articular and extra-articular fractures based on the involvement of the posterior facet of the subtalar joint as seen on multidetector CT scans.
· Intra-articular fractures: account for the majority of cases (70%–75%) and result typically from axial loading that produces shear and compression fracture lines.
- The fracture pattern depends on the position of the foot and the subtalar joint by the moment of the traumatism,
its force and the bone quality.
- There are many possibilities of fracture patterns; however,
an anteromedial and a posterolateral fragment are generally identified.
These fragments are created and split apart by the ‘primary fracture line’.
- The intra-articular fractures should be classified for an optimal evaluation.
- The best proved correlation to management and prognosis is found in the Sanders' classification system.
· Extra-articular fractures: account for 25%–30% of cases and include all fractures that do not involve the posterior facet and result from a variety of mechanisms. Generally,
extraarticular calcaneal fractures fall into one of three categories depending on whether the involvement of the calcaneus is anterior,
middle,
or posterior.
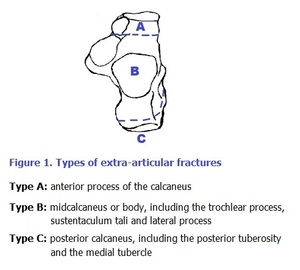
Fig. 1
Sanders classification
Classification system based on the number and location of articular fragments alone,
which they found to be useful in determining both treatment and prognosis after surgical management; several other authors have since found the system to be prognostic of outcome as well.
It is based on semi-coronal CT reformats and determined by the number and location of fracture lines through the posterior facet articular surface.
In general,
as the comminution of the posterior facet worsens,
the prognosis also worsens.
They arbitrarily selected the one image depicting the widest undersurface of the posterior facet of the talus (although the entire CT scan should be studied to follow fracture lines in and out of plane).
The talus is divided into three separate columns by two lines extending across the posterior facet of the calcaneus; a third line is added just medial to the medial edge of the posterior facet,
thus dividing the posterior facet of the calcaneus into three potential fragments: lateral,
central,
and medial.
These fragments,
plus the sustentaculum,
give a total of four potential articular fragments.
The fragments are then further subclassified by letter designation to denote the location of the primary fracture line from lateral to medial.

Fig. 2: Reference: Daftary A, Haims AH, Baumgaertner MR. Fractures of the calcaneus: a review with emphasis on CT. Radiographics. 2005 Sep-Oct;25(5):1215-26.
All nondisplaced (less than 2 mm) articular fractures are considered type I fractures,
regardless of the number of fracture lines.
Type II fractures are two-part fractures of the posterior facet,
with three possible subtypes: IIA,
IIB,
and IIC,
depending on the location of the primary fracture line.
Type III fractures are three-part fractures,
which typically include a centrally depressed fragment.
There are three possible subtypes: IIIAB,
IIIAC,
and IIIBC,
again depending on the location of the primary fracture line(s).
Type IV fractures are four-part fractures.
These are highly comminuted fractures and often have more than four articular fragments.
Although the subclassification of articular fragments has prognostic implications,
many surgeons elect to simply identify the number of articular fragments.
Overall,
the Sanders classification distinguishes between eight different possible fracture patterns
Regazzoni classification
The classification was developed through the analysis of 100 calcaneal fractures assessed by CT and it distinguishes between three main fracture types,
which are further divided into three subgroups: type A,
peripheral fractures (A1: extra-articular,
A2: avulsion fractures of the sustentaculum,
A3: fractures of the anterior process); type B,
fractures of the talocalcaneal joint (B1: posterior facet single,
B2: posterior facet multiple,
B3: tarsal sinus or middle or anterior facet); and type C,
fractures of the talocalcaneal and the calcaneocuboid joints (C1,
both joints single,
C2: one joint multiple or tarsal sinus,
and C3: both joints multiple),
resulting in a total of nine potential patterns of injury.
Each main group is divided into three subgroups (1,
2 and 3) according to fracture severity where 3 is the most severe.
The Regazzoni classification differs from other CT based classifications because it evaluates intra-articular fractures,
extra-articular fractures and the calcaneocuboid joint.
Therefore,
it is more accurate in detecting the lesions.

Fig. 3
In the following section we give some illustrative cases of patients with calcaneal fractures and their corresponding classification according to Sanders and/or Regazzoni:

Fig. 4
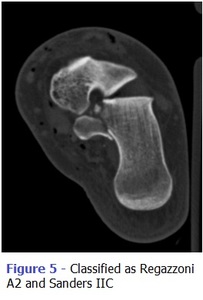
Fig. 5

Fig. 6
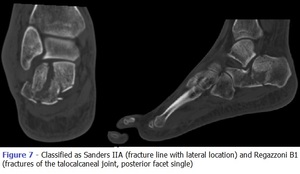
Fig. 7
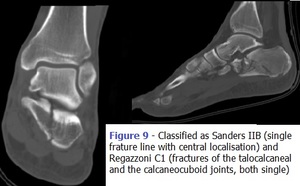
Fig. 8
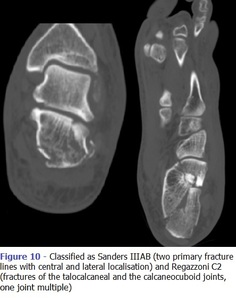
Fig. 9
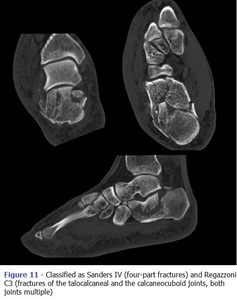
Fig. 10

Fig. 11
Complications
Early Complications
1. Swelling and Fracture Blisters
2. Wound Infection
3. Compartment Syndrome
4. Neurovascular Injury
Late Complications
1. Heel Pain and Heel Exostosis
2.Peroneal Tendon Tendinitis,
Peroneal Tendon Dislocation,
Flexor Hallucis Longus Tendon Injury
3. Malunion
4. Arthritis
Patient Related Complication
Poor prognostic factors include:
· Obesity
· Older than 50 years
· diabetes mellitus
· smoking
· drug addiction
· strenuous manual labor
Trauma Pattern Related Complication
Poor prognostic factors include:
· incongruity of the subtalar joint
· osteoarthritis of the talonavicular joint and ankle
· injury severity
