ACHILLES TENDON
The Achilles tendon is the strongest and largest tendon in the body (Figure 1).
It is the conjoined tendon of the gastrocnemius and the soleus muscles,
and may have a small contribution from the plantaris.
The muscles and the Achilles tendon are in the posterior,
superficial compartment of the calf.
Through the Achilles tendon,
they are the main plantar flexors of the ankle.
The Achilles tendon is subjected to the highest loads in the body,
with tensile loads up to ten times body weight during running,
jumping,
hopping,
and skipping.
This tendon is one of the most common sites of overuse injuries among athletes,
which ranges from inflammation of the peritendinous tissue (peritendinitis) or structural degeneration of the tendon (tendinosis) to partial or complete tendon rupture.

Fig. 1: Sagittal ankle MRI with fat supression shows Achilles Tendon (arrow).
ACHILLES
The most well-known tendon of the human body was named after Achilles (Fig.
2),
a hero in the Trojan War and the main character in the Iliad by Homer.
In 1693,
Philip Verheyen,
a Dutch surgeon,
was the first to actually name the Achilles tendon after the Greek hero.
Prior to that time,
it was known as the ‘‘tendo magnus of Hippocrates’’.
The terms achillobursitis,
achillodynia,
achillorraphy,
achillotenotomy and achillotomy are also derived from the name of our ancient hero.
Achilles was the son of Peleus,
king of the Myrmidons,
a tribe in Thessalia,
and the Nereid,
or sea nymph,
Thetis.
According to the story,
Achilles was raised by his mother,
Thetis,
who wanted to keep him safe for all eternity.
In an effort to make Achilles immortal,
Thetis dipped him in the River Styx,
but she didn’t want him to get swept away by the current,
so she held him by his heels.
Because his feet never touched the water,
he was only invincible above the heel.
Achilles became a great warrior.
The Trojan War broke out,
and with the help of Achilles,
the Greeks ravaged several cities around Troy over the first nine years of the war.
In the 10th year,
a quarrel with the Greek commander Agamemnon led Achilles to stop fighting.
Achilles’ closest friend,
Patroclus,
was struck down by Hector,
the eldest son of the King of Troy,
Priam.
Saddened and enraged that Patroclus had been killed,
Achilles challenged Hector to a battle,
and the Greek warrior came out victorious.
The war continued,
and Achilles became public enemy number one for Paris,
brother of Hector.
As the legend goes,
while the Greeks were attempting to take Troy,
Paris saw an opportunity to exact his revenge.
No other man had been able to strike down Achilles in battle,
so Paris readied a poison tipped arrow and drew his bow.
Guided by the god Apollo,
the arrow struck Achilles in the heel,
the spot where he was vulnerable.
The poison took hold,
and Achilles died a short while later.

Fig. 2: Statue of Achilles
References: internet
BICHAT'S LIGAMENT
Bichat´s ligament is the lower part of the dorsal sacroiliac ligament (fig.
3),
sometimes known as the transverse iliac ligament.
The long dorsal sacroiliac ligament has close anatomical relations with the erector spinae muscle,
the posterior layer of the thoracolumbar fascia,
and a specific part of the sacrotuberous ligament (tuberoiliac ligament).
Functionally,
it is an important link between legs,
spine,
and arms.
Pain localized within the boundaries of the long ligament could indicate among other things a spinal condition with sustained counternutation of the sacroiliac joints.
In diagnosing patients with aspecific low back pain or peripartum pelvic pain,
the long dorsal sacroiliac ligament should not be neglected.
Even in cases of arthrodesis of the sacroiliac joints,
tension in the long ligament can still be altered by different structures.
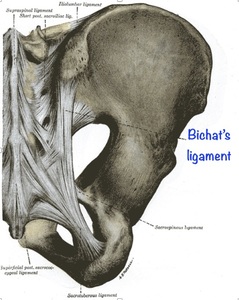
Fig. 3: Schematic drawing demonstrates Bichat´s ligament.
References: internet
MARIE FRANCOIS BICHAT
Marie François Xavier Bichat (Fig.
4) was a prominent French anatomist during a time of revolution and one of the founders of French scientific medicine.
Bichat was born in Thoirett,
Jura in 1771.
His father was Jean-Baptise Bichat,
a physician who had trained at Montpellier and was Bichat's first instructor.
Dr.
Bichat entered the college of Nantua,
and later studied at Lyon.
The revolutionary disturbances compelled him to flee from Lyon and take refuge in Paris in 1793.
There he became a pupil of P.J.
Desault. For two years he took active part in Desault's work,
at the same time pursuing his own research in anatomy and physiology.
At age 29 he was appointed as the chief physician to the Hotel-Dieu.
In 1796,
he and several other colleagues formally founded the Société d'Emulation de Paris,
which provided an intellectual platform for debating problems in medicine.
From 1799 onward he abandoned surgery and did only research in anatomy,
performing as many as 600 autopsies in a single year.
He investigated the structure of the body generally,
rather than studying particular organs as separate entities.
He broke down the organs into their common elemental materials,
for which he introduced the term "tissues."
He conducted several experimental studies,
which laid the foundation for modern physiology.
His name is carried on by several eponyms in anatomy and histology such as Bichat's fossa (pterygopalatine fossa),
Bichat's protuberance (buccal fat pad),
Bichat's foramen (cistern of the vena magna of Galen),
Bichat's ligament (lower fasciculus of the posterior sacroiliac ligament),
Bichat's fissure (transverse fissure of the brain) and Bichat's tunic (tunica intima vasorum).
He died at age 30,
fourteen days after falling down a set of stairs at Hotel-Dieu and acquiring a fever,
in 1802.

Fig. 4: Marie François Xavier Bichat
References: internet
BIGELOW'S LIGAMENT (iliofemoral ligament)
Bigelow's ligament (Figures 5 and 6) is very strong and shaped like an inverted Y,
lying anteriorly and intimately blended with the capsule.
Its apex is attached between the anterior inferior iliac spine and acetabulum rim,
its base to the intertrochanteric line.
The oblique lateral ligament attaches to a tubercle at the superolateral end of the intertrochanteric line,
the vertical medial ligament reaches the inferomedial end.
Parts of the ligament attached above and below the intertrochanteric line are thicker than the part attached to the central part of the line,
hence giving the inverted Y appearance.
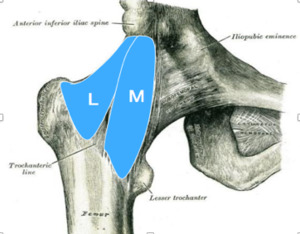
Fig. 5: Schematic drawing shows Bigelow’s ligament.
References: internet
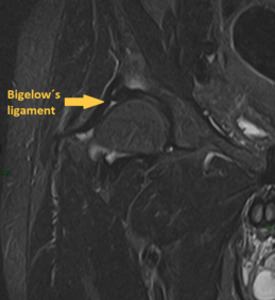
Fig. 6: Coronal MRI with fat supression of the right hip demonstrates Bigelow's ligament.
HENRY JACOB BIGELOW
Henry Jacob Bigelow (Fig.
7) was born in Boston in 1818.
Dr.
Bigelow was an American surgeon and Professor of Surgery at Harvard University.
A dominating figure in Boston medicine for many decades,
he is remembered for the Bigelow maneuver for hip dislocation,
a technique for treatment of kidney stones,
and other innovations.
His father,
Jacob Bigelow,
taught medicine at Harvard.
Bigelow entered Harvard College at fifteen years old and graduated in 1837.
He studied medicine both at Harvard and at Dartmouth College,
receiving his M.D.
at Harvard in 1841.
He was elected a Fellow of the American Academy of Arts and Sciences in 1846.
His "Insensibility during Surgical Operations Produced by Inhalation" (1846),
detailing the discovery of ether anesthesia,
was selected by readers of the New England Journal of Medicine as the "most important article in NEJM history" in commemoration of the journal's 200th anniversary.
Dr.
Bigelow described the structure and function of the Y-ligament of the hip joint in great detail,
and it still carries his name.
In 1878 he published "Lithotrity by a Single Operation",
in which he described his technique for "the crushing and removal of a stone from the bladder at one sitting." Prior to this,
surgeons would crush a bladder stone and then spend only a few minutes removing the pieces.
The remaining fragments would remain for a later session for removal.
This resulted in much discomfort and complications as the remaining fragments found an exit on their own.
Removing the entire bladder stone in one procedure was a great advancement.
Bigelow was professor of materia medica at Harvard from 1815 to 1855 and practiced medicine in Boston for sixty years.
He died on October 30,
1890 after an accident at his country home in Newton,
Massachusetts.
Fig. 7: Henry Jacob Bigelow.
References: internet
BOURGERY’S LIGAMENT (oblique popliteal ligament)
Bourgery's ligament or oblique popliteal ligament (OPL) (Fig.
8) is one of the five insertions of the semimembranosus muscle and forms part of the posterior anatomy of the knee.
It is a flat ligamentous band that arises from the lateral side of the semimembranosus muscle and posterior aspect of the tibial condyle.
It ascends obliquely laterally to attach to the medial surface of the lateral femoral condyle.
It blends with the posterior surface of the fibrous joint capsule and is the floor of the popliteal fossa.
This ligament stabilizes the posterior aspect of the knee joint and limits lateral rotation of the tibia.
This ligament is considered to be primary limiter of genu recurvatum and thus avoid hyperextension of the knee. Controlling knee hyperextension due to soft-tissue genu recurvatum is one of the functions of the posterior structures,
especially the OPL.
Hyperextension may alter gait and may lead to difficulty in walking across uneven ground.
Despite the great importance of the posterior structures of the knee,
including the OPL,
few studies in the literature have given emphasis to these structures,
because no techniques for reconstructing them have been described.
The OPL is not typically directly visualized on routine MR images.
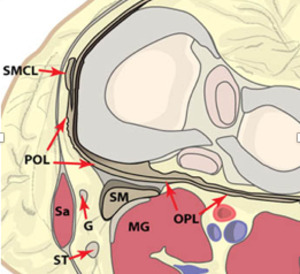
Fig. 8: An axial plane illustration of the knee at the level of the menisci demonstrates the components of the posteromedial corner. At this level the semimembranosus (SM) can be seen contributing fibers to the oblique popliteal ligament (OPL) and to the posterior capsule. The posterior oblique ligament (POL) is found between the superficial medial collateral ligament (SMCL) and the semimembranosus tendon on this view. The medial head of the gastrocnemius muscle (MG), sartorius muscle (SA), gracilis tendon (G) and semitendinosus tendon (ST) are also indicated.
References: internet
JEAN BAPTISTE MARC BOURGERY
Jean Baptiste Marc Bourgery (Fig.
9) was a French physician and anatomist who was a native of Orléans.
He was born in 1797.
In 1815 he began his studies in Paris,
where he attended courses given by naturalist Jean Baptiste Lamarck (1744–1829).
From 1817 to 1820 he worked as an interne at Parisian hospitals,
and subsequently spent several years as a medical officer at the copper foundries in Romilly-sur-Seine.
In 1827 he returned to Paris and received his medical doctorate.
In 1830 he began work on Traté complet de I'anatomie de I'homme comprenant la médecine operatoire,
a masterpiece on human anatomy that was published in eight volumes.
Bourgery worked on the atlas until his death in 1849,
with the last volume being published posthumously.
The finished work contained 2108 pages of folio-sized text and 726 hand-colored lithographs. It is considered to be one of the most comprehensive and beautifully illustrated anatomical works ever published.

Fig. 9: Jean-Baptiste Marc Bourgery.
References: internet
BRESCHET'S BONES
Brechet's bones or episternal ossicles (Figures 10 and 11) are retro- or supramanubrial accessory bones that result from supernumerary ossication centers.
They are found in 1.5% of the population.
Episternal ossicles may be unilateral or bilateral,
are pyramidal in shape,
and have a diameter of 2–15 mm.They are hard to identify on conventional radiographs but are clearly depicted on CT images,
where they must be distinguished from vascular calcications,
calci ed lymph nodes,
fracture fragments,
and foreign bodies.
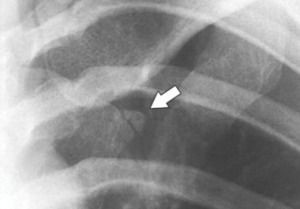
Fig. 10: Episternal ossicle. Collimated posteroanterior chest radiograph shows a small ossicle (arrow) lateral to the sternum.
References: internet

Fig. 11: Episternal ossicles. Axial chest CT image shows bilateral sternal ossicles (arrowheads).
References: internet
GILBERT BRESCHET
Gilbert Breschet (Fig.
12) was a French anatomist.
He was born on July 7,
1784 in Clermont-Ferrand.
Following his medical studies at the University of Paris,
he was conferred doctor of medicine at the University of Paris in 1812,
with a dissertation based on some of the thoughts of François Joseph Victor Broussais (1772-1838),
but worked over in a highly original way by Breschet.
After receiving his doctorate he settled in Paris.
He was chief of anatomical works at the Paris faculty.
In 1836 he was appointed professor of anatomy at the Faculté de Médecine de Paris.
Breschet made many contributions in comparative anatomy and in his research of zoonotic diseases.
In 1813 with François Magendie (1783–1855),
he demonstrated that rabies can be transmitted from the saliva of humans to dogs.
He did extensive anatomical studies of veins of the cranium and spine,
and made important investigations of the auditory system in vertebrates.
He provided a comprehensive description of the utricle and saccule of the  inner ear,
and is credited for introducing the terms "otoconia" and “helicotrema".
The helicotrema is sometimes referred to as "Breschet's hiatus",
a passageway that connects the scala tympani and scala vestibuli at the top of the cochlea.
inner ear,
and is credited for introducing the terms "otoconia" and “helicotrema".
The helicotrema is sometimes referred to as "Breschet's hiatus",
a passageway that connects the scala tympani and scala vestibuli at the top of the cochlea.
Breschet died in Paris on May 10,
1845.

Fig. 12: Gilbert Breschet.
References: internet
CHOPART’S JOINT
The midtarsal joint,
or Chopart joint (Figures 13,
14 and 15), is the articulation between the hindfoot (calcaneus and talus) and the midfoot (navicular,
cuboid and cuneiforms).
On lateral and AP views of the foot the talonavicular and calcaneocuboid joints are linked together by a smooth curved line also referred to as the cyma line.This line of demarcation is frequently used to separate the foot into two functional units: the hindfoot and forefoot.
Although these joints are biaxial,
they check each other reciprocally,
so that during motion each joint loses one of its axes of movement and a common uniaxial hinge joint results,
the transverse tarsal joint.
The midtarsal joint is named Chopart’s joint because Francois Chopart,
a French surgeon,
disarticulated this joint while performing amputations.

Fig. 14: Anteroposterior (AP) foot radiograph shows Chopart's Joint.
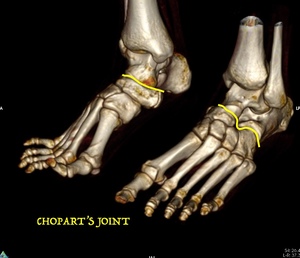
Fig. 13: CT of the feet. 3D reconstructions show both Chopart´s joints.

Fig. 15: Sagittal fat sat MRI of the ankle shows Chopart´s joint.
FRANÇOIS CHOPART
François Chopart (Fig.
16),
a native Parisian,
was the son of Francois Turlure and Marie-Anne Chopart,
whose name he took and used all through his life.
He received his medical training at the Hôtel-Dieu under Jean-Nicolas Moreau,
and at the Pitié and the Bicêtre.
In 1767 he received a prize from the Academy of Surgery for his treatise Essai sur les loupes.
In 1768 he received a prize for the treatise Memoire sur les lésions de la tête,
par contre-coup.
This was also the topic of his dissertation for the title of Maître de chirurgie,
which he received on July 20,
1770.
The following year he was appointed as professor of practical surgery at the école pratique.On March 13,
1782 he succeeded Toussaint Bordenave (1728-1782) in the chair of physiology.
François Chopart died in a cholera epidemic in 1795.

Fig. 16: François Chopart.
References: internet
DUPUYTREN'S FASCIA
Dupuytren's facia or palmar aponeurosis (Fig.
17) is a fibrotendinous complex that functions as the tendinous extension of the palmaris longus,
when present,
and as a strong stabilizing structure for the palmar skin of the hand.
It has five longitudinal slips that project into the base of each digit and a deeper transverse portion that crosses the palm at the proximal end of the metacarpals bones.
Dupuytren’s contracture is a relatively common disorder characterized by progressive fibrosis of the palmar fascia.
It is a benign,
slowly progressive fibroproliferative disease of the palmar fascia.
Initial fascial thickening is usually seen as a nodule in the palm,
which can be painful or painless and often goes unnoticed and undiagnosed.
Joint stiffness and a loss of full extension develop insidiously over decades.
The term Dupuytren disease is also used for this disorder,
as the fingers are not always held in a fixed flexion deformity.
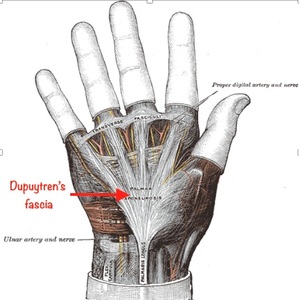
Fig. 17: Schematic drawing shows Dupuytren´s fascia (red arrow).
References: internet
GUILLAUME DUPUYTREN
The man who was to become one of the richest physicians in his time,
if not the richest,
was born in 1777 in the village of Pierre-Buffière,
near Limoges in the Haute Vienne district of central France,
where his father was an impoverished advocate.
After his time at school in Paris Dupuytren (Fig.
18) wanted to enter the army,
but in 1793,
at the insistence of his father,
he enrolled in the medical-surgical school of St.
Alexis Hospital in Limoges.
However,
he soon decided to pursue his education in Paris.
As a student Dupuytren for the next two years suffered hunger and desolation.
It is said that he lived in a garret and used fat from the cadavers in the dissecting room to make oil for the lamp by which he studied.
He attended classes at the Charité,
the Salpêtrière,
the École de Santé,
and the Collège de Magnac-Laval,
and by the time he graduated,
in 1797,
he had already caught the attention of the medical community in Paris.
In 1794,
Dupuytren obtained a post as prosector of the École de Santé,
where he gave anatomy lectures and was placed in charge of all the autopsies at the medical school,
and this laid a foundation for his future interest.
When he was 24,
in 1801,
he was appointed Chef des travaux anatomiques and soon had written a monograph on pathological anatomy based on his autopsy findings.
Already as a lecturer of anatomy Dupuytren introduced macroscopic pathology to surgery.
His acquisition of the doctorate of the University of Paris was delayed until
1803 as medical schools had been suppressed by the Revolutionary Government.
After qualification Dupuytren taught anatomy and at the age of 25 years,
through concours,
was appointed Chirurgien en second at the Hôtel-Dieu,
where he became a full member of the staff as Chief surgeon. Under his leadership the Hôtel-Dieu gained a leading position among the hospitals of Europe,
with Dupuytren reigning as chief of surgery for more than twenty years.
Dr.
Dupuytren never operated if an operation could be avoided,
but he was the first person to successfully remove the lower jaw.
He not only described Dupuytren contracture,
but devised an operation to cure it.
It was in 1831 - some four years before his death - that Dupuytren operated the contracture that bears his name. The operation consisted of fasciotomy - "la main du malade étant solidement fixée" - via traversing incision in vola and the little finger,
all described in detail,
including the postoperative swelling and the unavoidable wound infections.
After eight weeks the finger had «normal» movements.
In 1833 he had a stroke whilst lecturing,
but persisted and finished the lecture,
but from that time on he was an invalid.
In 1834 he had to withdraw from Hôtel-Dieu after more than 30 years of uninterrupted service,
and travelled to Italy.
On his return he resumed his work as a physician,
but his health failed ever more,
and he died in Paris two years later,
aged 58.

Fig. 18: Guillaume Dupuytren.
References: internet
GILULA’S ARC
Gilula's arcs (Figures 19 and 20) are three arcs connecting the proximal carpals.
The first arc is a smooth curve outlining the proximal convexities of the scaphoid,
lunate and triquetrum.
The second arc traces the distal concave surfaces of the same bones,
and the third arc follows the main proximal curvatures of the capitate and hamate.
The curves should be smooth.
Disruption of Gilula's lines may indicate carpal malalignment.

Fig. 19: PA hand radiograph with demarcation of Gilula´s arcs.
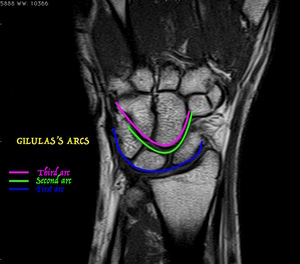
Fig. 20: Coronal T1-weighted MRI shows Gilula´s arcs.
LOUIS GILULA
Dr.
Louis Gilula (Fig.
21) was born in Lubbock,
Texas in 1942.
His life and career were dedicated to his three loves: his family,
his patients,
and his trainees.
Dr.
Gilula graduated from the University of Illinois School of Medicine (Chicago) with an MD degree and completed an internship at San Francisco General Hospital (San Francisco,
California).
From 1968 to 1970,
he served as a captain in the U.S.
Army.
After radiology residency at St Louis City Hospital (St Louis,
Mo),
in 1973,
he joined the Mallinckrodt Institute of Radiology,
Washington University School of Medicine,
where he rose to the rank of professor of radiology,
orthopaedic surgery,
and plastic and reconstructive surgery.
Dr Gilula headed the musculoskeletal section for 24 of his 40 years at Washington University.
He was an active member of multiple medical societies,
including the International Wrist Investigators Workshop,
for which he was a co-founder and the only radiologist member.
He was honored as a fellow of the American College of Radiology and was a winner of the Medal of the International Skeletal Society.
Dr.
Louis Gilula authored more than 300 peer-reviewed articles,
two textbooks,
and multiple chapters,
reviews,
and case reports.
His major contributions are in the wrist,
where “Gilula’s arcs” are still used to evaluate carpal alignment on radiographs.
Perhaps less well known is his pioneering work in interventional radiology.
He co-authored several early publications on angiography of arteriovenous fistulas used for hemodialysis and catheter-directed thrombolytic therapy.
He was also an early adopter and investigator of vertebroplasty and other image-guided percutaneous procedures for relief of chronic pain.
As important as the science,
Dr Gilula ensured that every patient received compassionate care.
Beyond his academic achievements,
Dr Gilula was most proud of his role as an educator.
At Mallinckrodt,
he was awarded the Distinguished Teacher of the Year Award in 2008.
Before his retirement,
a conference room was named for him.
Dr Louis A.
Gilula died on July 2,
2014,
after a battle with pancreatic cancer.
He was 71 years old.
Fig. 21: Louis A. Gilula.
References: internet
HESSELBACH'S LIGAMENT
Hesselbach's ligament (Fig.
22) or interfoveolar ligament is a thickening of the transversalis fascia extending from the inner edge of the inguinal ring upward along the inferior epigastric vessels,
toward the arcuate line. It sometimes contains a few muscular fibers.
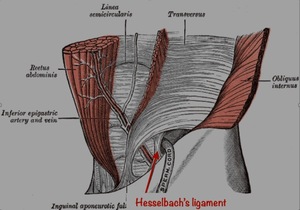
Fig. 22: Schematic drawing demonstrate Hesselbach´s ligament (red arrow).
References: internet
FRANZ KASPAR HESSELBACH
Franz Hesselbach was a German surgeon and anatomist who was a native of Hammelburg.
He was born in 1759.
Dr.
Hesselbach was a pupil,
and later Prosector under Karl Kaspar von Siebold (1736–1807) at Würzburg.
Later Hesselbach was a lecturer at Würzburg.
His son,
Adam Kaspar Hesselbach (1788–1856) was also a surgeon.
As a surgeon,
Hesselbach is best known for his work with hernia operations.
He was the first to describe a handful of anatomical structures,
such as the cribriform fascia (Hesselbach's fascia),
interfoveolar ligament (Hesselbach's ligament) and the inguinal triangle (Hesselbach's triangle).
Hesselbach died in 1816.
HOFFA'S FAT PAD
Hoffa´s fat pad (Figures 23 and 24) or infrapatellar fat pad is bordered by the inferior pole of the patella superiorly,
the joint capsule and patellar tendon anteriorly,
the proximal tibia and deep infrapatellar bursa inferiorly,
and the synovium-lined joint cavity posteriorly.
The fat pad is tethered to the intercondylar notch superiorly by the infrapatellar synovial fold or plica ligamentum mucosum.
It also is attached directly to the anterior horns of the menisci inferiorly and to the periosteum of the tibia.
This fad pad can be affected by a variety of pathologic conditions (lipoma,
hemangioma,
synovial chondromatosis,
focal villonodular synovitis,
ganglion cyst,
osteochondroma,
and chondrosarcoma).
Acute or repetitive trauma to the infrapatellar fat-pad can cause hemorrhage and inflammation of the pad and subsequent hypertrophy and predisposition to impingement between the femur and the tibia,
a condition known as Hoffa disease.
An increase in signal intensity and size of the infrapatellar fat-pad with accompanying mass effect on the patellar tendon represents a common pattern on fat-suppressed MR images in the acute phase of the disease.

Fig. 24: Lateral knee radiograph shows Hoffa's fat pad (arrow).
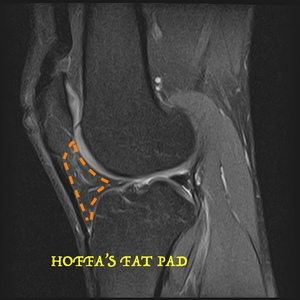
Fig. 23: Sagittal knee MRI with fat saturation shows Hoffa's fat pad.
ALBERT HOFFA
Albert Hoffa (Fig.
25) was a German surgeon,
orthopedist and physiotherapist born on March 31,
1859 in Richmond,
Cape of Good Hope.
He studied medicine at the Universities of Marburg and Freiburg,
earning his doctorate with a thesis on nephritis saturnina.
In 1886 he opened a private clinic for orthopedics,
physiotherapy and massage in Würzburg,
where in 1895 he became an associate professor at the university.
In 1902 he succeeded Julius Wolff (1836-1902) at the department of orthopedics in Berlin.
Hoffa is remembered for introducing an operation for congenital hip dislocations (1890),
as well as for development of a system of massage therapy (Hoffa system).
His name is associated with a condition known as "Hoffa's fat pad disease",
being characterized by chronic knee pain primarily beneath the patella.
In 1892 he founded the journal Zeitschrift fur orthopädische Chirurgie.
He died on December 31,
1907.

Fig. 25: Albert Hoffa.
References: internet
KAGER'S FAT PAD
Kager's fat pad (Figures 26 and 27),
also known as the pre-Achilles fat pad,
is a lipomatous structure located in the posterior ankle joint,
anterior to the Achilles tendon.
On lateral radiographs of the ankle,
Kager's fat pad is a sharply marginated,
radiolucent triangle.
The boundaries of the triangle are formed by three anatomic structures: the flexor hallucis longus muscle and tendon anteriorly,
the superior cortex of the calcaneus inferiorly,
and the Achilles tendon posteriorly.
The posterior ankle joint extends into the anteroinferior corner of this fat pad.
The retrocalcaneal bursa forms the posteroinferior corner of the pad.
Abnormal conditions involving the posterior ankle may result in increased and ill-defined soft-tissue density in Kager's fat pad or the obliteration or distortion of its borders.

Fig. 27: Lateral ankle radiograph shows Kager's fat pad (arrow).

Fig. 26: Sagittal ankle T1-weighted MRI shows Kager's fat pad.
HANS KAGER
Dr.
Hans Kager has a history that is hard to elucidate.
Besides his principal work (1939) on the treatment of Achilles tendon rupture,
no other publications of his were found.
From the original publication,
it can be derived that at the time,
he was working at the Hohenlychen Sanatorium in Lychen,
Germany.
Karl Gebhardt,
the Nazi doctor and personal physician of Heinrich Himmler,
who stood trial at the Nuremburg Doctors’ Trial and was sentenced to death for war crimes and crimes against humanity,
was the head of Dr.
Kager’s department.
In his original publication,
Kager mentions the triangle.
The term ‘‘Kager triangle’’ was first cited in a 1977 German publication.
The Kager triangle or Kager fat pad is also known as the preAchilles fat pad.
LIGAMENT OF ROUVIÈRE (CANELA LAZARO)
The fibulotalocalcaneal (FTC) ligament of Rouvière and Canela Lazaro (Figures 28 and 29) is an extrinsic ligament that occupies the posterolateral corner of the ankle and the posterior subtalar joints.
It originates from the medial border of the peroneal groove located on the posterior border of the lateral malleolus,
in common with the origin of the posterior talofibular (PTF) ligament,
and quite frequently may reach the origin of the calcaneofibular ligament.
This ligament may be continuous with the deep aponeurosis of the posterior lateral corner of the leg.
This flat structure is divided into two fibrous laminae: superomedial and inferolateral.
The inferolateral (peroneocalcaneal) lamina is the major component and inserts on almost the entire width of the superior surface of the calcaneus.
The other component inserts on the posterolat- eral tubercle of the talus.
The reported frequency of occurrence of this ligament is 60% as a well-defined ligament and 20% as a thin ligament having a weak structure but with a ligamentous texture.
It can be absent in 20% of persons and replaced by a thin fascia.

Fig. 28: Schematic drawing shows ligament of Rouviére (in red.
References: internet
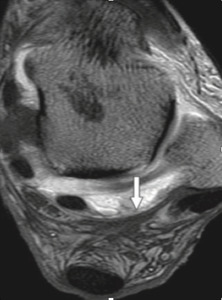
Fig. 29: Axial ankle MRI with fat supression demonstrates Rouvière´s ligament.
References: internet
HENRI ROUVIÈRE
In 1932,
Rouvière and Canela Lazaro described the fibulotalocalcaneal ligament,
also known as the “Rouvière ligament” or “ligamente of Rouvière and Canela Lazaro”.
Henri Rouvière (Fig.
30),
a French anatomist and embryologist,
was born in Le Bleymard,
(Lozère) France on December 23,
1875.
He studied medicine in Montpellier,
where he received his doctorate in 1903.
In 1910,
he became an associate professor of anatomy and embryology at the medical faculty of the University of Paris.
He became a full professor of anatomy at the same institute in 1927.
Rouvière is well known for the eponymous “node of Rouvière” (the most superior node of the lateral group of retropharyngeal lymph nodes).
This node is described in his 1932 publication,
Anatomie des Lymphatiques de I’Homme,
an extensive study describing and classifying the human lymph nodes and associated drainage regions.
Rouvière died on October 26,
1952.
Many of his anatomical works can be found in the Parisian Musée d’Anatomie Delmas Orfila-Rouvière.
Fig. 30: Henri Rouvière.
References: internet
LISFRANC'S JOINT
The Lisfranc joint complex (Figures 31 and 32) is composed of the tarsometatarsal (TMT) joints and the proximal intermetatarsal and anterior intertarsal joint articulations.
While little motion occurs at the joint articulations,
the complex is important in maintaining the structural stability of the midfoot.
The Lisfranc joint forms a shallow arc between the medial base of the second metatarsal and the lateral margin of the distal medial cuneiform,
a configuration that gives it little bony stabilization. The bony architecture of this joint,
specifically the “keystone” wedging of the second metatarsal into the cuneiform,
forms the focal point that supports the entire tarsometatarsal articulation.
Lisfranc joint injuries are very uncommon and often misdiagnosed.
Typical signs and symptoms include pain,
swelling and the inability to bear weight.
These injuries vary from mild sprains (typically in an athlete) to fracture-dislocations (as seen in motor vehicle accidents).
A Lisfranc fracture refers to a fracture-dislocation or fracture-subluxation of the tarsometatarsal joints,
typically the second through the fifth joints with lateral displacement of the metatarsals.
It is named for Lisfranc,
a surgeon in Napoleon’s army who described an amputation method through the tarsometatarsal joints.

Fig. 32: Anteroposterior (AP) foot radiograph shows Lisfranc's joint.

Fig. 31: CT of the feet. 3D images show Lisfranc´s joints.
LISFRANC'S LIGAMENT
The Lisfranc´s ligament (Fig.
33) is the medial (first) interosseous ligament,
and the largest of the three interosseous ligaments.
It is an oblique ligament that arises from the lateral surface of first cuneiform,
in front of the medial insertion of the intercuneiform ligament.
It extends distally,
laterally,
and slightly downward,
inserting on the lower half of the medial aspect of the second metatarsal.
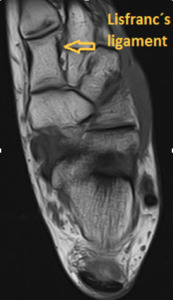
Fig. 33: Axial T1-weighted MRI of the ankle shows Lisfranc's ligament.
LISFRANC'S TUBERCLE
The upper surface of the body of the first rib is marked by two shallow grooves,
separated from each other by a slight ridge prolonged internally into a tubercle,
the scalene tubercle (Fig.
34) , for the attachment of the scalenus anterior; the anterior groove (groove for subclavian vein) transmits the subclavian vein,
the posterior (groove for subclavian artery) the subclavian artery and the lowest trunk of the brachial plexus.
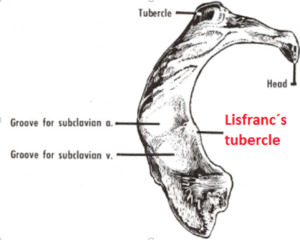
Fig. 34: Schematic drawing shows Lisfranc´s tubercle.
References: internet
JACQUES LISFRANC
Lisfranc (Fig.
35) was a French gynecologist and surgeon,
who was born on April 2,
1790,
in St.
Paul,
Loire.
Jacques Lisfranc began his surgical education in Lyon,
then went to Paris where he became an assistant to Guillaume Dupuytren (1777-1835),
and obtained his medical degree in 1813.
Following his promotion he was a short time active as an army surgeon,
but in 1814 left the army,
and from then on chiefly concerned himself with the improvement of surgical methods.
In 1826 two years after he had been habilitated he got his own department at L'Hôpital de la Pitié in Paris',
and soon commenced teaching clinical medicine.
Lisfranc devised many new operations including removal of the rectum,
lithotomy in women,
and amputation of the cervix uteri.
He concerned himself with operational treatments of fractures. In 1815,
with Champesme,
he described a method for the exarticulation at the shoulder joint.
Despite his recognition as a teacher and surgeon he was not a popular person,
his bellicose manners making any close friendships between him and his colleagues impossible.
He died on May 13,
1847.

Fig. 35: Jacques Lisfranc.
References: internet
PERKIN'S LINE
Perkin´s line (Fig.
36),
is the line drawn perpendicular to the Hilgenreiner line intersecting the lateral most aspect of the acetabular roof.
The upper femoral epiphysis should be in the inferomedial quadrant: it should lie below the Hilgenreiner line and medial to Perkin line.
These are used to diagnose DDH.
GEORGE PERKINS
George Perkins was born in Staines,
Middlesex,
in 1892.
He was educated at Hurstpierpoint College,
Sussex,
and Hertford College,
Oxford. He studied medicine at Oxford,
and St Thomas' Hospital,
London.
Perkins was awardedhis degree in 1916.
He was awarded the Military Cross for his services in East Africa.
He was also appointed to the Military Orthopaedic Hospital,
Hammersmith,
in 1919 and Senior Medical Officer at Shepherd's Bush Orthopaedic Hospital,
in 1920.
Dr.
Perkins became a Fellow of the Royal College of Surgeons,
in 1921,
and was elected honorary assistant surgeon to the Royal National Orthopaedic Hospital.
He returned to St Thomas' Hospital as Chief Assistant to the Orthopaedic Department in 1923,
and became Assistant Surgeon of the Department,
in 1926.
Perkins was recalled to the Army in 1939,
where he served in the Casualty Clearing Stations in France until 1940,
when he was invalided because of serious illness.
He began to write his book on fractures at this time and after his convalescence he worked at Queen Mary's Hospital,
Roehampton.
He became President of the British Orthopaedic Association.
In 1946,
he returned to St Thomas' and became head of the Orthopaedic Department,
a role he continued even when he was appointed Professor of Surgery in the London University at St Thomas' Hospital,
in 1948 until 1954.
He retired as head of the Orthopaedic department of St Thomas's in 1957.
He died in 1979.
HILGENREINER'S LINE
Hilgenreiner´s line (Fig.
36) is a line drawn horizontally through the superior aspect of both triradiate cartilages.
It should be horizontal and is mainly used as a measurement of the acetabular angle and as a reference for Perkin line.

Fig. 36: Anteroposterior (AP) pelvis radiograph shows Perkin's line (yellow) and Hilgenreiner's line (red).
HEINRICH HILGENREINER
Heinrich Hilgenreiner was a German surgeon and orthopedist.
He was born in Prague,
on November 3,
1870 and raised in a German family in Bohemia (which at the time was part of the Habsburg monarchy).
He served as a medical officer in the First World War.
After the war,
he became a professor of the German Charles-Ferdinand University in Prague and director of the Kinderklinik (children's clinic).
In 1946 he was forced to leave Czechoslovakia for Austria,
where he lived until his death.
He was the younger brother of Karl Hilgenreiner,
a theologian and politician,
also professor at Charles University.
He is the grandfather of the Austrian artist Gerhard Gleich.
He died in 1954 in Spillern,
Austria.
SHENTON'S LINE
Shenton's line (Fig.
37) is a smooth curvilinear line that is drawn along the inferior border of the superior pubic ramus and along the inferomedial border of the neck of the femur.
Interruption of the Shenton arc can indicate developmental dysplasia of the hip (DDH) or fractured neck of femur.

Fig. 37: Anteroposterior (AP) pelvis radiograph shows Shenton's line.
EDWARD WARREN HINE SHENTON
Edward Warren Hine Shenton (Fig.38) was an English radiologist.
He was born in 1872.
Shenton began his medical studies at Guy's Hospital in October,
1893.
While still a student he was employed as radiographer at Guy’s Hospital,
contemporaneously with A.
H.
B.
Kirkman.
The two collaborated to give a practical demonstration of the application of the Roentgen rays in medicine before the Pupils' Physical Society,
a report of which was printed in Guy's Hospital Gazette of November 4,
1899.
He made several original contributions to his specialty,
including a special apparatus for the detection of metallic foreign bodies,
and the excellence of his x-ray photographs became well known outside Guy's.
As a result,
he was in popular demand as a demonstrator of the then new science before local medical societies.
He resigned from the post of senior surgical radiographer at Guy's in 1919 because of the pressure of emergency work,
particularly his work as radiologist to the Royal Air Force Central Hospital.
For his distinguished services during the First World War he was awarded the Red Cross gold medal.
After the war Shenton developed his consultant practice in Harley Street,
and his fame and skill brought him much work.
In addition,
he was honorary radiographer to St.
Peter's Hospital.
From 1933 to 1950,
when he retired,
he was honorary radiologist to St.
Bartholomew's Hospital,
Rochester.
Shenton was elected an honorary member of the Trinity College of Music,
London,
in 1944.
He had a great zest for life and for work,
and he did not give up professional work until his 78th year.
He married Miss Phoebe Hollis in 1900,
and she collaborated in all his many activities.
He died in 1955.
Fig. 38: Edward Warren Hine Shenton.
References: internet
