Characteristic MRI appearances of mucoid degeneration
MRI is the gold standard modality for diagnosis of mucoid degeneration.
It is visualised as a bulky ligament with increased signal on all pulse sequences,
with ligament bundles and fibres readily distinguished on T2-weighted images (T2WI) and fluid sensitive sequences such as fat saturated proton density images (PDFS) but not well seen on T1-weighted images (T1WI)9 (Figure 1).
The characteristic feature of mucoid degeneration is a diffusely thickened ACL with intact ligamentous fibres spread apart by high signal intensity material (on T2WI/PD) giving a ‘celery stalk’ appearance3 (Figure 2) on sagittal sequences.
Table 1 details the main imaging features of mucoid degeneration.
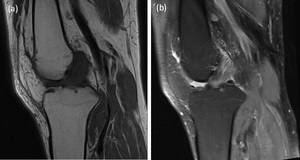
Fig. 1: Direct comparison of T1- weighted imaged (T1WI) (1a) and fat saturated proton density (PDFS) sequences (1b) in the same patient with mucoid degeneration demonstrates how the ACL bundles and fibres are better seen on PDFS compared to T1WI.
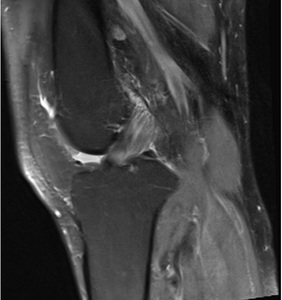
Fig. 2: The celery stalk sign is best seen on T2 weighted or PDFS images of the ACL. It is present when intact low signal longitudinal fibres are seen separated by higher signal mucinous material. The ligament retains a normal orientation.
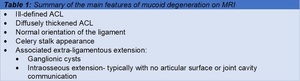
Table 1: Summary of the main features of mucoid degeneration on MRI
Confusion with partial ACL tears
The most important differential diagnosis of mucoid degeneration is a partial ACL tear.
In practice many cases of mucoid degeneration have been misdiagnosed as partial tears3; which can result in unnecessary investigation and intervention for the patient.
Both partial ACL tears and mucoid degeneration cause increased signal within the substance of the ACL3,10 (Figure 3).
On imaging mucoid degeneration shows no discrete disruption of the ACL fibres when viewed in all 3 planes (Figure 4) and lacks the indirect findings commonly associated with ACL injury including typical ACL pattern bone bruising (sulcus terminalis of the lateral femoral condyle,
posterolateral tibial condyle),
meniscal,
collateral ligament or osteochondral injuries,
anterior tibial subluxation3 (Figure 5).
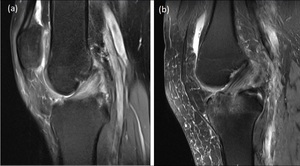
Fig. 3: Patients with mucoid degeneration (3a) have increased signal intensity present within the body of the ACL, which can appear similar to that which is present when a partial tear has occurred (3b).
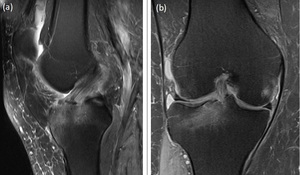
Fig. 4: Interrogation of a partial ACL tear in multiple planes. Both sagittal (4a) and coronal (4b) images show a discontinuity at the tibial insertion and extensive marrow oedema. Such features are consistent with a partial tear as opposed to mucoid degeneration.
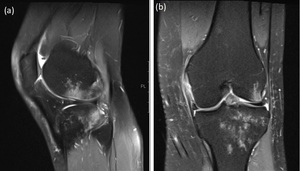
Fig. 5: A patient with bone bruising of the sulcus terminalis of the lateral femoral condyle and posterolateral tibial plateau (a) and associated complete tear of the medial collateral ligament near the proximal attachment (b) associated with ACL injury. Such findings are not present in the context of mucoid degeneration.
Clinical correlation is imperative when confidently differentiating ACL tears from ACL mucoid degeneration.
Typically,
mucoid degeneration lacks a strong trauma history or joint instability on examination.
Table 2 summarises the imaging and clinical differentiators between partial ACL tears and mucoid degeneration.
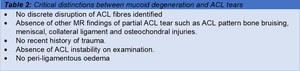
Table 2: Critical distinctions between mucoid degeneration and ACL tears
Differentiating mucoid degeneration from intra-ligamentous ganglion cysts
Another differential of mucoid degeneration is an intra-ligamentous ganglion cyst.
Clinically both pathologies are not associated with ligament instability and both lead to thickening of the ACL on MRI9.
Crucially the intrinsic signal intensity within the ACL in mucoid degeneration is not as bright as synovial fluid on fluid sensitive sequences9 (Figure 6).
Furthermore,
cysts tend to have a multi-loculated appearance which is not present in mucoid degeneration9.
There is an association between the two conditions and it is suggested they may be a continuum of the same degenerative process3,9.
Whilst they may occur independently of each other they frequently co-exist and often have similar associated features such as bone cysts,
erosions adjacent to bone and extra-ligamentous ganglion cysts9 (Figure 6).
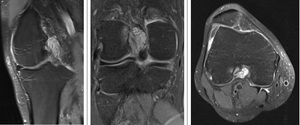
Fig. 6: Patient with co-existent ganglion cyst and mucoid degeneration. The ganglion cyst demonstrates typically bright signal intensity on PDFS equivalent to that of synovial fluid. The increased signal intensity of mucoid degeneration is less bright than that of the ganglion cyst.
