Chondroid matrix lytic bone lesions (chondroid matrix usually identified as rings and arcs or popcorn calcifications),
most of them benign,
can show some symptoms and radiologic findings that make us think of possible malignancy.

Fig. 1: Chondroid matrix. Enchondroma
General features of enchondromas and osteochondromas,
findings raising concern for malignancy and chondrosarcoma features will be discussed
Enchondroma:
Centrally located,
they can grow until skeletal maturity.
Chondral calcifications will usually be seen,
except in short tubular bones (phalanges) where they can be pure lytic lesions.

Fig. 2: Lytic enchondroma in finger
Common benign findings in enchondromas:
-Subtle endosteal scalloping
-Cortical expansion
-Pathologic fracture

Fig. 3: Subtle endosteal scalloping (less than 2/3) is not suspicious for malignancy

Fig. 4: Cortical expansion is not suspicious for malignancy
Malignant transformation is more common in multiple enchondromas síndromes:
- Ollier disease: multiple enchondromatosis mainly in a single shortened limb
- Maffucci syndrome: multiple enchondromatosis with multiple soft tissue hemangiomas
However,
there are some other signs uncommon in enchondromas,
which should raise concern for a possible chondrosarcoma:
-Pain (in absence of pathologic fracture): Think of malignancy until proven otherwise
-Deep endosteal scalloping (beyond 2/3 of the cortical thickness) would be the best differential finding for some authors (1).
A longitudinally extensive scalloping would be less specific7 8.
Must be assessed by CT or MRI
-Cortical breach
-Cortical thickening or periostic reaction
-Soft tissue mass: Typical in chondrosarcoma.
Excludes the possibility of enchondroma9
-Permeative pattern
-Size beyond 5 cm
-Increased heterogeneous uptake on bone scan

Fig. 5: Cortical breach in this chondrosarcoma

Fig. 6: Periostic reaction in chondrosarcoma
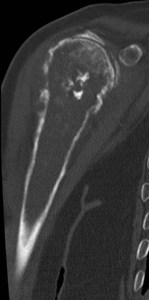
Fig. 7: Periostic reaction in chondrosarcoma

Fig. 8: Periostic reaction in chondrosarcoma

Fig. 9: Periostic reaction and soft tissue mass in chondrosarcoma
Osteochondroma:
It is a bone exostoses sessile or pedunculated coming from the metaphysis (with cortical and medullar continuity with main bone) and growing towards the diaphysis.
The lesions is coated by cartilaginous tissue

Fig. 10: Pedunculated osteochondroma

Fig. 11: Sessile osteochondroma
They grow until skeletal maturity.
After that,
the cartilage cap can go on growing slowly until the patient is 30 years old.
They commonly produce no pain,
but sometimes they do due to nerve or vessel compression,
bursitis,
peducle fracture o avascular necrosis of the cartilaginous cap.
Signs which should raise concern for possible malignancy in osteochondromas:
-Pain after puberty
-Cartilage cap thickness over 2 cm.
Assessed by CT
-Lesion growth (or increased uptake in bone scan) after skeletal maturity
-Growth towards the epiphysis
-Scattered calcifications in the cartilage cap
-New onset cortical breach or irregularity.
-Soft tissue mass
Risk for malignant transformation is under 1%,
but it grows with the number and size of osteochondromas.
Sessile osteochondromas suffer from malignant transformation more often.
Hereditary multiple exostoses (with autosomal dominant inheritance) has a higher risk for malignant transformation

Fig. 12: Hereditary multiple exostosis. Multiple osteochondromas

Fig. 13: Hereditary multiple exostosis. Multiple osteochondromas
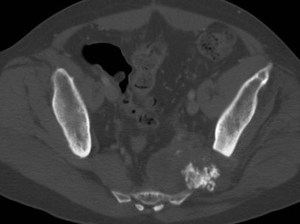
Fig. 14: Chondrosarcoma in a patient with hereditary multiple exostoses.
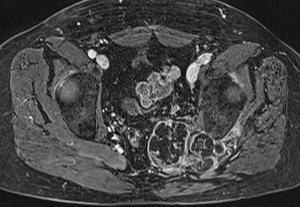
Fig. 15: Chondrosarcoma in a patient with hereditary multiple exostoses.
Chondrosarcoma:
It’s the third most common primary bone malignancy (after multiple myeloma and osteosarcoma)
Chondrosarcomas arise in flat bones or long bones (in metaphysis and diaphysis)
Findings are of a lytic mass with or without condroide matrix,
that produces cortical expansion and thinning (or sometimes thickening).
It can show cortical discontinuity and a commonly calcified soft tissue mass.

Fig. 16: Chondrosarcoma arising from a rib
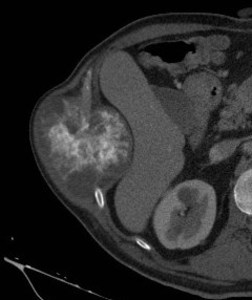
Fig. 17: Chondrosarcoma arising from a rib
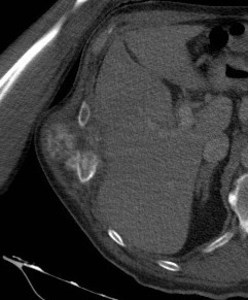
Fig. 18: Chondrosarcoma arising from a rib
They can be primary (90%) or secondary to malignant transformation of enchondromas and osteochondromas,
these last with lower grade and better prognosis.
Conventional chondrosarcoma:
Centrally and medullary located,
usually in long bones.
Pain is the most common symptom,
usually progressive,
longstanding and with night worsening.
Upper grade chondrosarcomas have less chondroid matrix (less calcifications) and more cellularity (more enhancement).
The most aggressive lesions show a permeative or moth-eaten pattern
Yuxtacortical chondrosarcoma:
Much less common,
in young patients (3rd and 4th decades of life).
Usually they present as a slow growing painless palpable mass.
Located in long bones surface (most commonly in the posterior distal femur)
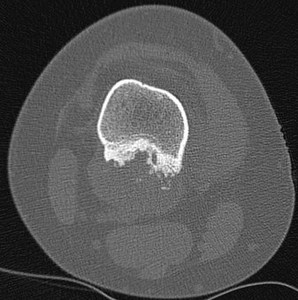
Fig. 19: Yuxtacortical chondrosarcoma. It is often similar in imaging to yuxtacortical chondroma
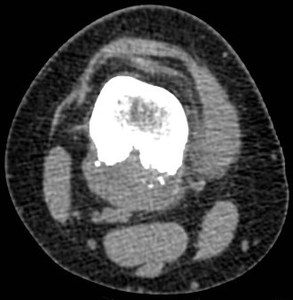
Fig. 20: Yuxtacortical chondrosarcoma. It is often similar in imaging to yuxtacortical chondroma
CT or MRI would show a lobulated soft tissue mass in the bone surface,
producing erosion and adjacent cortical erosion and thickening,
with Codman triangles in the lesion margins.
Medullar infiltration is rare.
This tumor is pathologically and radiologically similar to yuxtacortical chondroma.
The best way to differenciate them would be the size,
chondroma being smaller (2-3 cm),
and chondrosarcoma being bigger (3-14 cm).

 is not suspicious for malignancy")