BRACHIAL PLEXUS
INTRODUCTION
Brachial plexus is the main sensory and motor innervation of the upper extremity.
It may be involved in a variety of traumatic and nontraumatic pathologies.
Brachial plexus injury (BPI) is the most severe nerve injury of the extremities,
resulting in functional impairment of the upper limb.
Various space-occupying lesions,
such as hematoma,
nerve sheath tumors,
benign tumors,
primary or secondary tumors of perineural spaces,
and various tumor variants (diffuse polyneuropathies) may involve the different elements of the brachial plexus.
Benign peripheral nerve sheath tumors include neurofibroma,
schwannoma (encapsulated,
displaces the nerve fascicles),
and ganglioneuroma (an elongated lobulated lesion along the ganglion chain).
The therapeutic measures for BPI depend on the pathologic condition and the location of the injury and both ultrasound and MRI are useful in diagnosis and in localization of these lesions.
Imaging studies play an essential role in differentiating preganglionic injuries from postganglionic lesions,
a differentiation that is crucial for determining the management of BPI.
With respect to preganglionic injuries,
functions of some denervated muscles are restored with nerve transfers.
Postganglionic lesions are repaired with nerve grafting or followed up conservatively.
ANATOMY
The brachial plexus is formed by the ventral roots of C5 to T1 nerve roots (Fig.1).
These unite to form three trunks which split into three anterior and three posterior divisions.
They unite to form the three cords that further divide into five peripheral nerves.
The roots and trunks are supraclavicular in location while divisions are retroclavicular and the cords are infraclavicular.
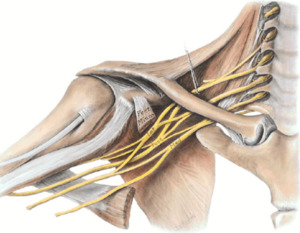
Fig. 1: Schematic drawing. Right brachial plexus.
References: internet
The brachial plexus contains both anterior (motor) and posterior (sensory) rootlet fibers.
The first portion of the plexus,
called roots,
is named for the level from which they arise (C5–C8,
T1).
The axial plane best shows the anterior and posterior rootlets and the roots exiting the neural foramina.
Note that each root is subdivided into preganglionic and postganglionic portions,
which are demarcated by the dorsal root ganglion (Fig.
2).

Fig. 2: Schematic drawing. Brachial plexus anatomy.
References: internet
SITES OF ENTRAPMENT
Sites of entrapment include the retropectoralis minor,
costoclavicular,
and interscalene spaces.
CAUSES
NONTRAUMATIC PLEXOPATHY
Nontraumatic brachial plexopathy can be from a localized mass effect or a more widespread inflammatory process.
Masses include primary and secondary tumors and nonneoplastic processes such as aneurysms and cervical ribs.
Primary tumors arising from the nerves are seen in younger patients.
These neoplasms may be sporadic and benign (e.g.,
schwannoma) or may result from a condition (e.g.,
neurofibromatosis type 1) with a genetic predisposition for both benign and malignant lesions (e.g.,
neurofibroma and malignant peripheral nerve sheath tumor).
A cervical rib (Fig.
3) is a unique cause of brachial plexopathy in that the cause of a patient’s symptoms can be detected on conventional radiography.
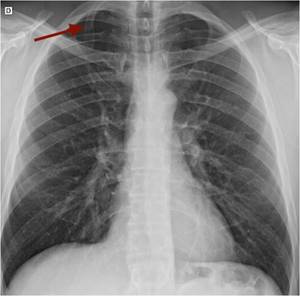
Fig. 3: Chest PA radiograph. Right cervical rib (arrow).
Thoracic outlet syndrome
Thoracic outlet syndrome involves the brachial plexus and the subclavian artery or vein at three specific anatomic levels where they are vulnerable to entrapment: the interscalene space,
the costoclavicular space,
and the retropectoralis minor space.
Abducting the arm narrows the thoracic inlet in the costoclavicular and retropectoralis minor spaces.
This syndrome may result from posttraumatic fibrosis of the scalene muscles,
compression secondary to activities like backpacking,
and clavicular fractures with abundant callus formation.
Exercise related causes presumed secondary to muscle hypertrophy affect weight lifters,
swimmers,
and athletes involved in “dominant arm sports” such as tennis.
Other causes include mass lesions such as lipomas,
neurogenic tumours,
accessory muscles,
and fibrous bands.
Sagittal T1- weighted MR imaging sequences are particularly useful in demonstrating the presence of denervation-related fatty atrophy of muscles,
effacement of fat planes around the compressed plexus,
and an abnormal intramuscular course of the components of the brachial plexus.
The retropectoralis minor space is not frequently affected by entrapment and is more often involved by mass lesion.
Parsonage-Turner syndrome
There are several synonyms for the term Parsonage-Turner syndrome,
including acute brachial neuritis and neuralgic amyotrophy.
The cause of Parsonage-Turner syndrome is unknown however,
reports have postulated localized infectious or immunologic disorders,
with a possible genetic predisposition.
This syndrome occurs mostly in the 3rd to 7th decades of life and is more common in males.
Symptoms include severe atraumatic shoulder pain followed by significant weakness of one or more shoulder muscles.
In this syndrome,
although MR imaging does not adequately demonstrate the involved nerve,
denervation injury causes diffuse high signal in the involved muscles,
which becomes evident at T2-weighted imaging within 2–4 days.
With chronic denervation over a period of months,
muscle atrophy may be identified at T1-weighted imaging,
with or without fatty infiltration.
A diagnosis of Parsonage-Turner syndrome is suggested at MR imaging when there is no history of trauma or excessive overhead activity.
A history of antecedent viral illness can sometimes be elicited.
Multiple nerves may be involved.
Suprascapular nerve involvement is seen in nearly all cases (97%) and axillary nerve involvement is common (50%).
It has been reported that the supraspinatus muscle is most frequently involved,
followed (in order of decreasing frequency) by the infraspinatus,
deltoid,
teres minor,
and subscapularis muscles.
Multiple entities may resemble Parsonage-Turner syndrome because denervation edema and muscular atrophy are nonspecific findings.
Mimics may include trauma,
quadrilateral space syndrome,
and myositis.
MR imaging (Fig.
4) aids in determining which nerves are involved,
while simultaneously excluding common mimics.
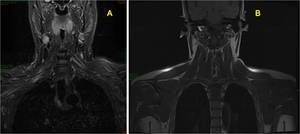
Fig. 4: Normal brachial plexus MRI. (A) Coronal STIR and (B) Coronal T1.
PRIMARY NEOPLASMS
Neurogenic Tumors
Primary neurogenic tumors of the brachial plexus can be benign or malignant and include neurofibroma,
plexiform neurofibroma (Fig.
5) ,
schwannoma (Fig.
6 and 7) ,
and malignant peripheral nerve sheath tumor.

Fig. 5: (A) Coronal and (B) sagittal T2-weighted chest MRI images show soft tissue masses involving brachial plexus bilaterally, the posterior mediastinum an multiple neural foramina. Plexiform neurofibromas in a patient with neurofibromatosis type 1.
Neurofibromas are the most common neural tumor to involve the brachial plexus.
Histologically,
these lesions are unencapsulated tumors believed to arise from the nerve fascicles.
One-third of these lesions occur in patients with neurofibromatosis type 1,
whereas two thirds of cases are sporadic.
These tumors are characteristically multiple and plexiform in appearance,
with diffuse involvement of the brachial plexus in patients with neurofibromatosis.
The imaging features of solitary neurofibromas overlap those of schwannomas,
and often they are indistinguishable.
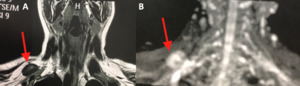
Fig. 6: MRI of brachial plexus. (A) T1-weighted image. Coronal plane. (B) Diffusion Coronal plane. Nodular hypointense lesion in contact with the upper aspect of the right brachial plexus. Nerve sheath neoplasm.
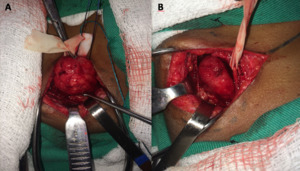
Fig. 7: Intraoperative photograph shows tumor representing nerve sheath neoplasm. Courtesy of Souza FH, Hospital da Restauração – Recife-PE, Brazil
At CT,
both neurofibromas and schwannomas have attenuation similar to that of muscle and both demonstrate variable amounts of enhancement with contrast material.
At MR imaging,
both lesions are isointense to muscle on T1-weighted images and hyperintense on T2-weighted images and may have central areas with low signal intensity,
the so-called target sign.
Neurofibromas and schwannomas enhance intensely after administration of gadolinium-based contrast material.
Malignant peripheral nerve sheath tumors develop in 3%–13% of patients with neurofibromatosis.
These tumors are also known as neurofibrosarcomas,
neurogenic sarcomas,
malignant neurofibromas,
and malignant neurilemomas and occur most commonly in patients with neurofibromatosis type 1,
especially after radiation therapy.
The imaging features of malignant neural tumors overlap those of their benign counterparts,
making differentiation between the two challenging.
Findings that favor a malignant neural tumor include large size,
irregular margins,
and heterogeneity.
Clinically,
the finding of a progressively enlarging mass in a patient suggests a malignant nerve sheath tumor.
Benign Tumors
Many benign tumors occur along the course of the brachial plexus and involve or impinge on its various components.
In our series,
benign tumors included neurofibromas,
desmoid tumors,
lymphangiomas,
and lipomas (Fig.
8).
A wide range of other benign tumors (Fig.
9) has been reported in the literature.
Although the appearance of many benign processes is nonspecific,
some offer imaging.
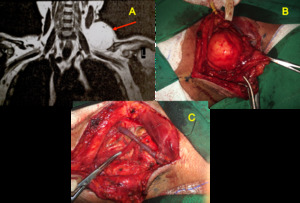
Fig. 8: (A) Brachial plexus MRI. 52-year-old man. Coronal T1-weighted image shows soft tissue mass with fat component in the left supraclavicular region (arrow), between the sternocleidomastoid, trapezium and supraspinatus muscles involving the upper trunk of the left brachial plexus. (B) and (C) Intraoperative photographs demonstrate the mass and after its removal respectively.
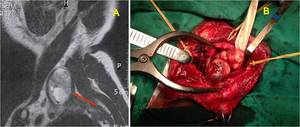
Fig. 9: A) Brachial plexus MRI. Sagittal image shows a heterogeneous soft tissue mass in the left supraclavicular region. Benign neoplasm.(B) Intraoperative photograph of the mass. Courtesy of Souza FH, Hospital da Restauração – Recife-PE, Brazil
SECONDARY NEOPLASMS
Direct Invasion
Primary tumors of the lung,
bone,
on soft tissues in the neck,
the supraclaviculan fossa,
on the upper part of the thorax may directly invade the brachial plexus.
Superior sulcus carcinoma (Pancoast’s tumor) is an uncommon form of bronchogenic carcinoma that arises in the lung apex.
The tumor may invade locally into ribs,
vertebral bodies,
subclavian yessels,
and the brachial plexus.
The ability of MR to image in coronal and sagittal planes facilitates visualization of the tumor and its relationship to adjacent structures.
Metastasis
Metastatic disease to lymph nodes,
soft tissue,
on bone can involve the brachial plexus and manifest as a focal mass or diffuse infiltration.
Because the lymphatic drainage of the breast is through the apex of the axilla,
it is not uncommon for recurrent or metastatic breast carcinoma to invade the brachial plexus.
Intraspinal metastases may extend through the neural foramina and involve nerve roots.
Lymphoma can similarly affect the brachial plexus.
TRAUMATIC PLEXOPATHY
There are two distinctive populations affected by traumatic brachial plexopathy.
The first is neonates who have sustained a traction injury due to shoulder dystocia during vaginal delivery.
This trauma leads to a flaccid ipsilateral upper extremity.
The second population affected by traumatic brachial plexopathy is young men in the second and third decades.
These patients sustain blunt force injury after a fall from a height or a motorcycle or motor vehicle crash and penetrating injury from a gunshot.
Given the forces involved with these mechanisms,
recognition of these injuries may be delayed because of concomitant injuries to the head or spine that draw attention away from the brachial plexus.
Therefore it is essential for the radiologist to identify causes of brachial plexopathy that can be ameliorated in the early posttrauma period before irreversible nerve damage and muscle atrophy occur.
ENTRAPMENT AT THE SHOULDER
MUSCULOCUTANEOUS NERVE
ANATOMY
The musculocutaneous nerve (Fig.10) arises from the lateral cord of the brachial plexus and contains fibers from the C5,
C6,
and C7 spinal nerve roots.
However,
the most important contributions come from the C5 and C6 levels.
It supplies the coracobrachialis,
brachialis,
and biceps brachii muscles,
while providing cutaneous innervation to the lateral forearm.
In the axilla,
the musculocutaneous nerve courses laterally away from the axillary artery,
pierces (and supplies) the coracobrachialis muscle and descends towards the elbow between biceps brachii and brachialis muscles.
In the cubital fossa,
it courses lateral to the biceps tendon as the lateral cutaneous nerve of the forearm,
which is simply the sensory continuation of the musculocutaneous nerve after it has distributed all its motor fibres in the anterior compartment of the arm.
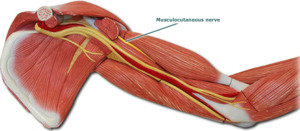
Fig. 10: Schemamtic drawing shows musculocutaneous nerve.
References: internet
SITES OF ENTRAPMENT
Sites of entrapment include the coracobrachialis muscle and the point of emergence of the lateral antebrachial cutaneous nerve.
Weakness of biceps brachii muscle and,
sometimes,
sensory deficit in the forearm are the main symptoms of musculocutaneous neuropathy.
CAUSES
Musculocutaneous nerve entrapment is relatively rare and tends to be posttraumatic.
Proximal to the elbow,
the nerve is susceptible to entrapment at or just distal to the coracobrachialis muscle,
usually producing weakness of the brachialis and biceps brachii muscle.
The lateral antebrachial cutaneous nerve is vulnerable to entrapment where it pierces the antebrachial fascia in the cubital fossa.
External compression of the nerve against the biceps brachii tendon,
as well as repetitive and vigorous arm exercise,
may result in entrapment.
Isolated musculocutaneous nerve injuries are rare and the reported causes are penetrating traumas,
anesthetic blocks,
anterior shoulder surgery especially in coracoid abutment (Latarjet procedure),
and sport related entrapment such as windsurfing,
rowing or weightlifting athletes.
Proximal nerve injury can occur when the nerve pierces the coracobrachialis muscle during violent extension of the arm in throwing athletes or by entrapment between the biceps brachii and the brachialis muscles,
in forced abduction and external rotation. Imaging,
especially ultrasound,
can be useful to assess the nerve after surgical procedure,
and to exclude cervical radiculopathy.
CLINICAL FEATURES
Injury to the musculocutaneous nerve manifests as weakness involving the muscles it innervates.
Entrapment at or just distal to the coracobrachialis muscle typically produces symptoms in all the innervated muscles except the coracobrachialis muscle.
Sensory abnormalities mimicking lateral epicondylitis are present in the lateral aspect of the forearm.
There appear to be two clinically distinct syndromes involving this nerve,
a lesion of the musculocutaneous before its division into the lateral cutaneous nerve,
causing a mixed motor and sensory syndrome,
and a lesion of the sensory portion,
which causes pure sensory findings of the lower radial aspect of the volar forearm.
The lateral cutaneous nerve syndrome is characterized by numbness in the radial half of the volar forearm with some diffuse tenderness over the elbow crease just lateral to the insertion of the biceps tendon.
Compression of the nerve proximally at the level of the coracobrachialis muscle manifests with pain and weakness of the biceps brachii and dysesthesia over the radial side of the forearm.
RADIOLOGIC FINDINGS
MR imaging is better for assessing injury or entrapment of the musculocutaneous nerve at the level of the coracobrachialis muscle.
Although the nerve itself may not be visualized easily at MR imaging,
edema within the coracobrachialis,
brachialis,
and brachioradialis muscles suggests involvement of the nerve.
Entrapment of the lateral antebrachial cutaneous nerve at its point of emergence from the lateral aspect of the biceps muscle can be demonstrated dynamically with US.
AXILLARY NERVE
ANATOMY
The axillary nerve (Fig.
11) originates from the posterior cord of the brachial plexus giving muscular branches to teres minor and deltoid.
It also supplies the shoulder joint and the skin over it.
Proximally,
it runs below the coracoid process and along the anterior surface of the subscapularis muscle.
It then turns toward the inferior aspect of the shoulder joint and courses through the quadrilateral space,
traveling around the posterolateral humeral surgical neck and dividing into anterior and posterior branches.
The anterior branch innervates the anterior and middle portions of the deltoid muscle.
The posterior branch divides into the upper lateral brachial cutaneous nerve and the nerve to the teres minor muscle.
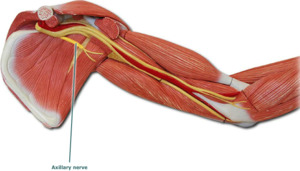
Fig. 11: Schematic drawing demonstrates axillary nerve.
References: internet
The quadrilateral space is bounded laterally by the medial aspect of the humerus,
medially by the long head of the triceps muscle,
superiorly by the teres minor muscle,
and inferiorly by the teres major muscle.
The axillary nerve is most commonly injured (6% of all the brachial plexus injuries) during numerous orthopaedic surgeries like shoulder arthroscopy,
thermal shrinkage of the shoulder capsule (excessive temperature) and plate fixation (retraction of deltoid muscle) of the proximal humerus.
The shoulder joint dislocation and rotator cuff tear causes nerve injury which is called “unhappy triad” of the shoulder joint.
The axillary nerve is vulnerable to damage during acute trauma to the shoulder or by chronic repeated trauma like in ‘quadrilateral space syndrome’ (entrapment of axillary nerve).
There is an increased risk of nerve injury during intramuscular injections in deltoid,
intra-articular and intra-bursal steroid injections due to lack of proper anatomical knowledge of the nerve.
It is very much necessary to appreciate the exact anatomical location of the nerve and its course to avoid the possible damages and to protect the nerve during surgeries and injections.
SITES OF ENTRAPMENT
Sites of entrapment include the quadrilateral space and the area anteroinferior to the glenohumeral joint.
CAUSES
Extrinsic compression by hematoma,
posteroinferior labral cyst,
bone callus,
tumour,
and accessory subscapularis muscle are other common etiologies of axillary nerve injury.
Most axillary nerve injuries are secondary to brachial plexus impairment.
A common cause of isolated injury is open surgical intervention with a deltoid muscle–splitting approach.
Entrapment can occur while one is exercising or is maintaining the arm in a prolonged abducted and externally rotated position,
such as during sleep.
Posttraumatic nerve injury may occur in up to 45% of shoulder dislocations,
since the nerve is stretched over the dislocated humeral head.
This injury occurs just proximal to the quadrilateral space.
Chronic compression of the axillary nerve,
known as quadrilateral space syndrome is a rare and misdiagnosed neurovascular syndrome.
Quadrilateral space syndrome
This syndrome is defined as compression or mechanical injury of the axillary nerve or posterior circumflex artery as they pass through the quadrilateral space.
Quadrilateral space syndrome has both traumatic and atraumatic causes,
and typically affects young,
active individuals.
The nerve can be affected by mass lesions such as tumors,
posteroinferior paralabral cysts,
or fibrous bands,
with fi brous bands being the most frequently implicated.
Osteoarthritis of the glenohumeral joint may cause compression or traction of the nerve resulting from large osteophytes.
CLINICAL FEATURES
The clinical diagnosis of axillary nerve injury is challenging because signs and symptoms are vague.
Pain is poorly localized over the anterior aspect of the shoulder,
with potential radiation to the arm and forearm.
Paresthesia of the skin over the upper lateral brachial cutaneous nerve or weakness of the deltoid muscle can be expected.
Posttraumatic nerve injury secondary to shoulder dislocation may be masked clinically by pain.
Athletes may experience fatigue,
particularly with heavy weight lifting and overhead activities.
Atrophy of the teres minor and deltoid muscles may be visualized later in the course of the disease.
Imaging can play an important role in detecting the underlying causes of nerve damage by showing extrinsic mass,
or deltoid or teres minor muscles denervation sign.
It should also be noticed that about 50% of Parsonage-Turner cases affect the axillary nerve and thus this diagnosis must be kept in mind.
RADIOLOGIC FINDINGS
Radiographs are useful in ruling out a proximal humeral fracture or severe degenerative changes,
and in evaluating the adequacy of shoulder reduction following dislocation.
At MR imaging,
the axillary neurovascular bundle is surrounded by fat and is well seen be- low the inferior glenoid rim.
MR imaging is useful for the detection of masses or other pathologic conditions of the shoulder.
Indirect evidence of axillary nerve dysfunction may take the form of edema in the teres minor muscle or,
less commonly,
the deltoid muscle.
If isolated edema or atrophy of the teres minor or deltoid muscle is detected in the absence of a quadrilateral space mass,
signs of glenohumeral instability should be sought.
SUPRASCAPULAR NERVE
ANATOMY
The suprascapular nerve is a sensorimotor nerve that arises from the upper trunk of the brachial plexus and is formed by the ventral rami of C5 and C6 roots and occasionally from the C4 root. Then,
it crosses the posterior cervical triangle in the supraclavicular fossa,
deep to the omohyoid muscle.
It travels obliquely across the posterior triangle of the neck toward the coracoid process.
Medial to the coracoid process,
it courses through the suprascapular foramen,
which is formed by the suprascapular notch and the transverse scapular ligament.
The suprascapular nerve then enters the supraspinatus fossa and supplies the supraspinatus muscle.
Finally,
it curves around the spinoglenoid notch beneath the transverse scapular ligament and supplies the infraspinatus muscle.
The suprascapular nerve is a mixed nerve providing motor innervation to the supraspinatus and infraspinatus muscles and sensory innervation of the coracohumeral ligament,
the coracoclavicular ligament,
the subacromial bursa,
the acromioclavicular joint and upper and posterior glenohumeral joint.
SITES OF ENTRAPMENT
Sites of entrapment include the suprascapular notch and the spinoglenoid notch.
CAUSES
The site of suprascapular nerve entrapment determines whether the infraspinatus muscle alone or both the infraspinatus and supraspinatus muscles are affected.
The causes of the nerve entrapment are multiple.
The suprascapular notch is the most frequent point for the suprascapular nerve to be entrapped by compression or traction.
In addition,
the anatomic configuration of the suprascapular notch may represent a predisposing factor to the development of entrapment.
Other predisposing factors are uncommon narrow or closed notches and the ossification of the transverse suprascapular ligament,
the latter being related to aging.
Extrinsic compression by labral or mucoid cyst,
tumour or varicose enlargement of the suprascapular veins,
is another common cause of nerve entrapment.
Fractures of the suprascapular notch,
or posterior fracture dislocation of the humeral head,
have been associated with lesions of suprascapular nerve.
Microtraumatisms by repetitive movements,
especially with overhead activities,
for example in volleyball and baseball athletes,
expose the nerve to tension especially with a predisposing anatomy.
CLINICAL FEATURES
Suprascapular nerve syndrome
This syndrome commonly occurs with repetitive strain on the abducted and externally rotated shoulder,
leading to a thickened transverse scapular ligament.
Compression from space-occupying lesions,
including paralabral cysts,
tumors,
iatrogenic surgical injury,
and enlarged varicosities,
is also common.
It often manifests with motor loss and insidious onset of deep,
generalized,
dull posterior shoulder pain.
Functional motor loss is often minimal.
Although patients with chronic suprascapular nerve compression often have atrophy of both the supraspinatus and infraspinatus muscles,
physical examination tends to help identify only the loss of infraspinatus muscle volume,
since the supraspinatus muscle is obscured by the bulk of the trapezius muscle.
RADIOLOGIC FINDINGS
Edema and atrophy of the supraspinatus and infraspinatus muscles may be seen in suprascapular notch syndrome at MR imaging.
In spinoglenoid notch syndrome,
only the infraspinatus muscle tends to display abnormal signal.
Imaging,
especially MRI,
plays an important role to detect the underlying causes of nerve damage (extrinsic mass,
rotator cuff tear,
etc.),
the precise topography of injury (involvement of both supraspinatus and infraspinatus muscles if the nerve is injured at suprascapular notch and isolated denervation sign of infraspinatus muscle if the nerve is injured distally to suprascapular notch).
MRI is also useful to determine the severity of the nerve injury (edema and/or atrophy) and to diagnose other cause of neuropathy such as cervical radiculopathy or Parsonage-Turner syndrome.
The suprascapular nerve is involved frequently.
Bilateral or multiple involvements of muscles without relevant trauma or sport activities or heterogeneous patterns of muscle signal on MRI are important clues for ruling out Parsonage-Turner syndrome.
Recently,
Sneag et al.,
reported the MRI bullseye sign as an indicator of peripheral nerve constriction in Parsonage-Turner syndrome.
ENTRAPMENT AT THE ARM AND ELBOW
RADIAL NERVE
ANATOMY
The radial nerve (Fig.
12) arises from the posterior cord of the brachial plexus (C5 through C8,
T1),
follows the brachial artery dorsally,
twists around the humerus,
crosses under the teres major muscle,
and then descends between the medial and lateral bellies of the triceps muscle.
After this it courses through the spiral groove of the humerus (1).
This structure innervates the triceps,
brachioradialis,
extensor carpi radialis,
and supinator muscles,
as well as the skin along the posterior upper arm.
About 10 cm proximal to the lateral epicondyle,
this nerve crosses from the dorsal aspect of the upper arm to the volar aspect of the elbow through the lateral intermuscular septum.
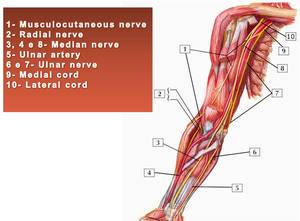
Fig. 12: Schematic drawing shows upper limb nerves anatomy.
References: internet
SITES OF ENTRAPMENT
Sites of entrapment include the spiral groove and the lateral head of the triceps muscle.
CAUSES
The most common site of nerve compression is at the proximal edge of the supinator muscle.
CLINICALFEATURES
A proximal radial neuropathy in the spiral groove leads to functional loss of accessory forearm supination,
elbow flexion,
wrist and digital extension,
and thumb abduction,
as well as sensory loss in the dorsolateral hand.
Patients may present with pain in the proximal forearm and tenderness in the nerve at the level of the supinator muscle.
RADIOLOGIC FINDINGS
Usually,
the radial nerve can be detected easily on axial T1-weighted images as a low-signal-intensity structure at the elbow joint,
where the nerve courses between the brachialis and brachioradialis muscles.
Acute or subacute radial neuropathy manifests with diffuse increased signal intensity on T2-weighted MR images in all or some of the muscles supplied by the radial nerve.
Signal abnormalities in more proximal muscles such as the triceps,
extensor carpi radialis longus,
and anconeus muscles are consistent with high radial nerve entrapment.
ULNAR NERVE
ANATOMY
The ulnar nerve arises from the medial cord of the brachial plexus (C8 and T1).
The nerve follows the brachial and axillary artery medially and downward to the midportion of the humerus.
This nerve may pass under the arcade of Struthers,
which is present in 70% of individuals and is situated 8 cm proximal to the medial epicondyle.
The nerve follows a groove in the medial head of the triceps muscle,
arriving at the cubital tunnel.
This fibro-osseous interval is formed anteriorly by the medial epicondyle and laterally by the olecranon.
The roof is formed by the arcuate ligament.
SITES OF ENTRAPMENT
Compression of the ulnar nerve may occur at four different locations along its course at the elbow from proximal to distal: at the intermuscular septum due to the arcade of Struthers, at the medial epicondyle at the entrance to the cubital tunnel,
within the cubital tunnel and at the flexorpronator aponeurosis between the heads of the flexor carpi ulnaris as the nerve enters the forearm.
CAUSES
Cubital tunnel syndrome is the second most common peripheral neuropathy of the upper extremity (1),
arises from pathologic compression or a lesion of the ulnar nerve within the cubital tunnel,
where the nerve passes beneath the cubital tunnel retinaculum (also known as the epicondylo-olecranon ligament or Osborne band).
Others causes of compression include an anconeus epitrochlearis muscle,
osteophytes,
ganglia,
synovitis,
laxity of the ulnar collateral ligament,
and tardy ulnar nerve palsy.
Figures 13 and 14 show tumor involving the ulnar nerve.
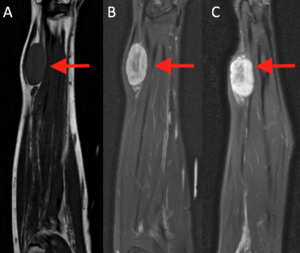
Fig. 13: MRI of the forearm. (A) Coronal T1 weighted image, (B) coronal PD SPIR and (C) sagittal PD SPIR demonstrate a well demarcated lesion involving the distal right ulnar nerve. Nerve sheath tumor.
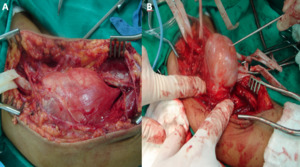
Fig. 14: (A)and (B) Intraoperative photographs show tumour (schwannoma).
Courtesy of Souza FH, Hospital da Restauração – Recife-PE, Brazil
CLINICAL FEATURES
Patients with ulnar neuropathy complain of pain,
paresthesias,
and weakness in the fifth finger and ulnar side of the fourth finger and numbness in the dorsal ulnar aspect of the hand and fingers.
Chronic compression may lead to claw deformities of the fourth and fifth fingers and to loss of grip.
RADIOLOGIC FINDINGS
MRI of the symptomatic ulnar nerve may show signal hyperintensity on T2-weighted images and nerve swelling,
but signal hyperintensity is not a specific finding because it has been shown in 60% of asymptomatic elbows.
Ultrasound has also shown nerve enlargement in ulnar neuropathy (Fig.
15 and 16 ) with some authors advocating comparison with the patient's contralateral asymptomatic nerve and others advocating a ratio of the cross-sectional area at the location of maximal nerve swelling to the cross-sectional area at a nonswollen location.
Care must be taken to image the contralateral elbow or other locations in the ipsilateral elbow in the same amount of elbow flexion because the cross-sectional area of the nerve decreases with flexion.
In addition,
the nerve may have multiple separate fascicles that must be evaluated additively.
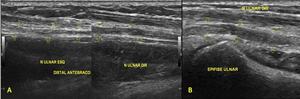
Fig. 15: Ultrasound images (A,B) show hypoechoic and thickened ulnar nerve in the forearm. Focal inespecific ulnar neuritis.(C) Contralateral forearm.
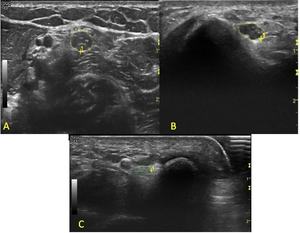
Fig. 16: Ultrasound images show inespecific ulnar neuropathy.
RADIAL NERVE AND POSTERIOR INTEROSSEOUS NERVE AT THE ELBOW
ANATOMY
At the level of the elbow joint,
the radial nerve divides into a superficial,
sensory branch that courses in the forearm along the deep surface of the brachioradialis muscle and a deep motor branch that enters the radial tunnel.
The radial tunnel extends from the level of the radiocapitellar joint to the level of the proximal aspect of the supinator muscle and is bounded by the joint capsule posteriorly,
the brachialis muscle and biceps tendon medially,
and the brachioradialis muscle and the extensor carpi radialis brevis and longus muscles laterally.
At the distal aspect of the radial tunnel,
the deep branch pierces the supinator muscle anteriorly between the superficial and deep heads of the supinator and exits the posterior aspect of the supinator muscle as the posterior interosseous nerve to enter the posterior compartment of the forearm.
At the elbow,
the deep branch supplies the extensor carpi radialis brevis muscle and the supinator muscle,
and in the posterior compartment of the forearm,
the deep branch,
now called the posterior interosseous nerve,
supplies the extensor carpi ulnaris,
extensor digitorum communis,
extensor digiti minimi,
abductor pollicis longus,
extensor pollicis longus and brevis,
and extensor indicis proprius muscles.
SITES OF ENTRAPMENT
Sites of entrapment include the level of the radial head by fibrous bands between the brachioradialis muscle and joint capsule,
distal to the radial head by the leash of Henry,
the level of the tendinous edge of the overlying extensor carpi radialis brevis muscle,
the arcade of Frohse along the proximal aspect of the supinator muscle and the distal aspect of the supinator muscle.
CAUSES
Posterior interosseous nerve syndrome occasionally is caused by overuse (eg,
in athletes or in violinists),
external compression (eg,
due to use of crutches),
radial head fracture,
soft-tissue tumors such as ganglion,
lipoma,
septic arthritis,
synovial chondromatosis,
or rheumatoid synovitis.
Figures 17 and 18 show multiple neuropathies in a patient with Hanseniasis.
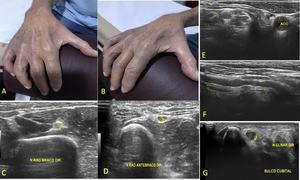
Fig. 17: Patient with Hanseniasis. (A) and (B) photographs of the patient´s hand demonstrate atrophy. Ultrasound images (C, D, E, F,and G)show diffuse thickening of upper limb nerves.
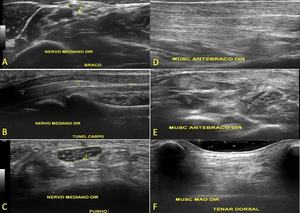
Fig. 18: Ultrasound images of the same patient with Hanseniasis demonstrate volume loss and increased echogenicity of the muscles of the right forearam and hand.
CLINICAL FEATURES
Radial tunnel syndrome causes pain over the anterolateral proximal forearm in the region of the radial neck,
without motor loss.
This syndrome is often clinically difficult to distinguish from lateral epicondylitis.
In addition,
lateral epicondylitis and radial tunnel syndrome are simultaneously present in 7% of patients.
Approximately 5% of patients in whom recurrent “tennis elbow” is initially diagnosed may actually have radial tunnel syndrome.
RADIOLOGIC FINDINGS
The posterior interosseous nerve may be depicted with high signal intensity on T2-weighted fat-suppressed or STIR images.
In patients with posterior interosseous nerve syndrome,
direct visualization of a compressive anatomic structure is seldom possible at MR imaging.
Occasionally,
the arcade of Frohse may be seen as a low-signal-intensity band at the proximal edge of the supinator muscle.
However,
the diagnosis of posterior interosseous nerve syndrome is based primarily on the muscle denervation pattern,
which may indicate the level of the nerve lesion.
In general,
a proximal lesion affects all muscles innervated by the radial nerve,
whereas a more distally located lesion may spare muscles that are innervated by motor branches given off more proximally to the lesion.
In a typical case of posterior interosseous nerve syndrome in which muscle weakness is the leading symptom,
the supinator,
extensor digitorum,
extensor carpi ulnaris,
extensor digiti minimi,
abductor pollicis longus,
extensor pollicis brevis,
extensor pollicis longus,
and extensor indicis muscles may have abnormal signal intensity,
while the extensor carpi radialis muscle is spared.
The exact site of the lesion in such cases may be determined even without direct visualization of the anatomic structure that compresses the posterior interosseous nerve.
MEDIAN NERVE AND ANTERIOR INTEROSSEOUS NERVE AT THE ELBOW
ANATOMY
The median nerve arises from the medial and lateral cords of the brachial plexus (C6 through C8,
T1).
The nerve follows the axillary artery and lies superficial to the brachial muscle in the upper arm.
It lies between the humeral (superficial) and ulnar (deep) heads of the pronator teres muscle at the level of the elbow joint.
At the elbow and proximal aspect of the forearm,
the median nerve supplies the pronator teres,
flexor carpi radialis,
palmaris longus,
and flexor digitorum superficialis muscles.
SITES OF ENTRAPMENT
Sites of entrapment include distal humerus by the ligament of Struthers, proximal elbow by a thickened biceps aponeurosis,
elbow joint between the superficial and deep heads of the pronator teres muscle,
which is the most common cause of median nerve compression and proximal forearm by a thickened proximal edge of the flexor digitorum superficialis muscle.
CAUSES
The anterior interosseous nerve may be compressed by the pronator teres muscle and by the proximal edge of the flexor digitorum superficialis muscle as well as along its course in the forearm by masses or other space-occupying processes.
It can also be dynamically compressed by repetitive elbow flexion or forearm pronation.
The median nerve may be injured by a supracondylar spur and Struthers ligament,
supracondylar fracture,
elbow dislocation,
injection injury,
or pronator syndrome.
Figure 19 demonstrates interosseous nerve injury.
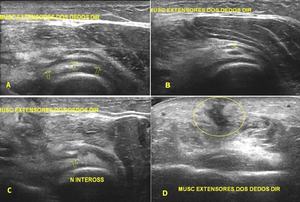
Fig. 19: Penetrating injury by sharp object resulting in tear of extensor muscles and posterior interosseous nerve. Short (B and C) and long (A and D) axis ultrasound images show scar (yellow circle in D), posterior interosseous nerve (arrows in A, B and C) and almost all extensor muscles with edema and bruise.
CLINICAL FEATURES
Patients with pronator syndrome have pain and paresthesia in the volar aspects of the elbow and forearm and in the hand affecting the first through third digits and lateral half of the ring finger.
Patients with anterior interosseous nerve syndrome,
also called the Kiloh-Nevin syndrome,
present motor weakness typically manifested by weakened ability to pinch the thumb and index finger together,
tested by asking the patient to make an “OK” sign with the hand,
reflecting the palsy of the flexor pollicis longus muscle and flexor digitorum profundus muscle to the index finger.
RADIOLOGIC FINDINGS
In pronator teres syndrome,
the median nerve may appear normal or may demonstrate abnormal signal intensity at MR imaging.
The denervation pattern at MR imaging (including muscle edema or atrophy) is crucial for diagnosis.
With median nerve symptoms,
US is useful in two scenarios.
First,
it can reveal dynamic compression of the nerve deep to the bicipital aponeurosis that is not demonstrable with MR imaging.
Second,
it is valuable in cases of suspected median nerve laceration.
ENTRAPMENT AT THE WRIST
ULNAR NERVE
INTRODUCTION
Nerve entrapment syndromes in the hand and wrist involve the median nerve in carpal tunnel syndrome,
ulnar nerve in Guyon canal syndrome (ulnar tunnel syndrome),
and the ulnar digital branch of the radial nerve in bowler´s thumb.
ANATOMY
The ulnar nerve runs through the forearm deep to the flexor carpi ulnaris muscle in its proximal course and lateral to the muscle distally.
At the wrist,
it passes lateral to the pisiform bone and courses through the Guyon canal along with the ulnar artery.
In the Guyon canal,
it divides into superficial sensory and deep motor branches.
After coursing around the hamate hook,
it passes posteriorly through the hypothenar muscle,
crossing the deep palm to end at the adductor pollicis muscle.
The Guyon canal is partitioned into three zones as defined in terms of the ulnar nerve bifurcation: zone 1 consists of the area proximal to the bifurcation,
whereas zones 2 and 3 encompass the deep and superficial branches of the bifurcated nerve.
The deep motor branch supplies the hypothenar muscles,
adductor pollicis muscle,
third and fourth lumbrical muscles,
and all the interosseous muscles.
SITES OF ENTRAPMENT
Sites of entrapment include the Guyon canal and the tendinous arch of the adductor pollicis muscle.
CAUSES
In the Guyon canal,
the nerve is stretched around the pisohamate ligament with hand extension,
making it vulnerable to external compression or laceration.
Chronic repetitive trauma involving the use of tools,
bicycle handlebars (cyclist’s palsy),
or crutches is a common cause of entrapment
The most common cause of compression is a ganglion originating from the pisotriquetral joint (Fig.
20).
However,
there are case reports of midpalmar ganglia from the second or third carpometacarpal joints and intercarpal joint.
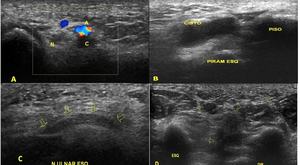
Fig. 20: Short axis with color Doppler (A) and long (B and C) axis ultrasound images show pisotriquetral cyst close to a thickened ulnar nerve (N in A and arrows in C) within Guyon canal. In D short axis images compare hypothenar muscles atrophy and normal muscles on the right.
Compression may be secondary to lipomas,
cysts,
pisotriquetral joint osteoarthrosis,
os hamuli proprium (a congenital anomaly of the hamate hook),
or anomalies of ligaments or muscles such as an accessory abductor digiti minimi muscle,
accessory or reversed palmaris longus muscle and anomalous hypothenar adductor muscle.
Fractures of the pisiform bone or hamate hook can also cause compression.
CLINICAL FEATURES
Guyon canal syndrome
In this syndrome,
symptoms depend on the site of the lesion in regard to the ulnar nerve bifurcation.
The most common lesion (type 1 lesion) is found in a site proximal to the Guyon canal and is characterized by sensory loss combined with weakness of all ulnar intrinsic hand muscles.
Type 2 syndrome is characterized by weakness of all the ulnar intrinsic hand muscles without sensory loss,
with isolated compression of the deep motor branch as it leaves the Guyon canal in the region of the hamate hook.
Type 3 syndrome manifests with sensory loss over the volar surface of the hypothenar eminence and the ulnar two digits with deep branch sparing.
This manifestation is secondary to an isolated lesion of the superficial branch and is most commonly caused by an ulnar artery aneurysm,
thrombosis,
or hamate hook fracture.
Physical examination typically reveals tenderness during percussion over the ulnar nerve at the wrist,
particularly in patients in whom sensory fibers of the ulnar nerve are affected.
Weakness or atrophy of intrinsic hand muscles also may be present,
depending on the site of the lesion and the corresponding muscle denervation pattern.
Decreased strength during pinching and gripping,
and an abduction deformity of the small finger (also known as Wartenberg sign of the ulnar nerve),
also may be observed.
T1-weighted sequences are best suited for identifying the ulnar nerve within the Guyon canal.
On T1-weighted images,
the nerve appears as a round or ovoid structure surrounded by a small amount of fat.
The bifurcation of the ulnar nerve normally is well depicted,
and the course of both branches can be followed distally.
MR imaging may help exclude the presence of a mass lesion and may demonstrate compression by an anomalous or accessory muscle or fibrous band.
Furthermore,
MR imaging is an excellent method for detecting abnormalities in the intrinsic hand muscles.
Carpal tunnel syndrome (CTS)
Compression of the median nerve as it courses through the carpal tunnel,
is the most common entrapment neuropathy in the body.
Although some studies have suggested that the prevalence of CTS may be as high as 3% or 4% in some populations,
most believe that it has a prevalence of approximately 2% of the adult population in the United States,
affecting 4–10 million patients.
The carpal tunnel (Fig.
21) is an enclosed fibroosseous space formed by volar aspects of the carpal bones dorsally and the flexor retinaculum volarly.
The flexor retinaculum is a mildly convex volar fibrous structure that stretches between the tip of the hook of the hamate and the pisiform medially and the trapezium and scaphoid laterally.
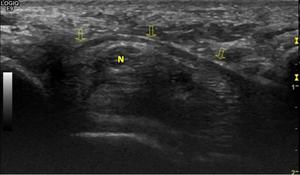
Fig. 21: The transverse carpal ligament (arrows) forms the roof of the carpal tunnel. N =median nerve
The carpal tunnel encompasses nine tendons (the four flexor digitorum superficialis tendons,
four flexor digitorum profundus tendons,
and flexor pollicis longus tendon) and the median nerve,
which lies along the volar superficial aspect of the tunnel.
The median nerve (Fig.
22) provides sensory and motor innervation to the thumb,
index finger,
third digit,
and radial half of the fourth digit.
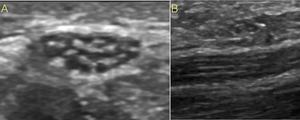
Fig. 22: Normal nerve echotexture. (A) Short axis and (A) long axis ultrsound images of median nerve in the wirst show hypoechoic spots (fascicles) embedded in a hyperechoic epineurium)background.
Clinically,
patients complain of nocturnal pain,
hand clumsiness,
tingling,
and numbness in the median nerve distribution.
Typically,
sensory loss precedes motor deficit.
Patients with longstanding disease may have wasting of the soft tissues in the thenar eminence on physical examination.
Entrapment of the nerve within the carpal tunnel can result from an abnormality that decreases the size of the canal or that enlarges the contents of the canal.
Increased canal contents are most often idiopathic but also can result from a wide variety of abnormalities,
such as space-occupying lesions including ganglion cysts,
fibrolipoma of the median nerve,
or anomalous muscles in the tunnel (Fig.
23),
synovial hypertrophy related to inflammatory arthritis,
such as rheumatoid arthritis,
deposition of foreign materials,
such as amyloid or systemic diseases that cause nonspecific enlargement of the contents of the tunnel,
such as congestive heart failure and inborn errors of metabolism.
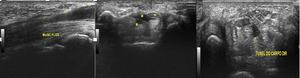
Fig. 23: Carpal tunnel flexor muscle (anatomic variant) Ultrasound images. Nerve (N) and M (muscle).
Figure 24 illustrates median nerve normal variant and figures 25 to 32 demonstrate different median nerve pathologies.
Video (33) shows median nerve tumor.
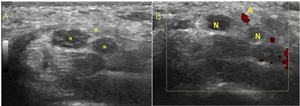
Fig. 24: Persistent median artery and bifid median nerve. Transverse gray-scale and e color Doppler images obtained at the proximal carpal tunnel demonstrate the median artery (A) located between the radial and ulnar trunks (N) of a bifid median nerve.
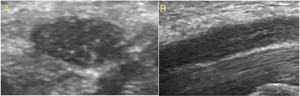
Fig. 25: Hypoechoic median nerve. Short axis e long axis ultrasound images of median nerve show reduced echogenicity due to edema of the fascicles and of the epineurium causing loss of the fascicular echotexture.
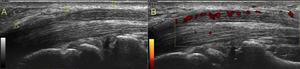
Fig. 26: Entrapment neuropathy. Long-axis ultrasound image of the median nerve at the carpal tunnel level (A) reveals an abrupt change in the size of the nerve at the proximal edge of the retinaculum. The nerve is flattened within the carpal tunnel and markedly swollen proximal to the level of compression (notch sign).
B Long-axis color Doppler US image of the median nerve in the same patient with carpal tunnel syndrome demonstrate flow signals within the median nerve.
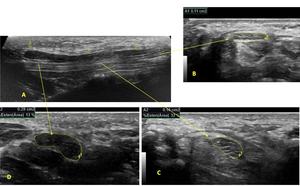
Fig. 27: Hypoechoic and thickened median nerve within and after carpal tunnel. Long (A) and short axis (B, C and D) ultrasound images show median nerve and its measurements.
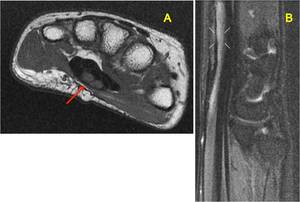
Fig. 28: Median nerve neuritis. (A) axial T1 and (B) sagittal PD fat sat.
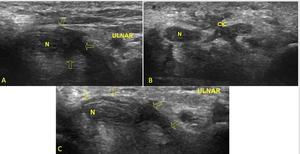
Fig. 29: Ultrasound images of postoperative encasement of nerves by scar tissue. (A) Median nerve (N), scar tissue involving the median nerve (arrows). (B)Median nerve (N) and cicatricial tissue (cic). (C)Ulnar side, median nerve (N)and cicatricial tissue (arrows).

Fig. 30: MRI of the wrist. Coronal A,B and C)and axial (F, G, H and I)show complete tear of the median nerve, retinaculum and flexor tendons
Intraoperative photographs (D) and (E) before and after repair of median nerve and flexor tendons.Courtesy of Ayala A, MD Recife, Brazil.

Fig. 31: Penetrating injury by a sharp object compromising the radial nerve and complicated by two neuromas. Ultrasound in (A) shows normal radial nerve in the forearm. Images (B) and (C) demonstrate hypoechoic fibrous tissue as the result of such a disorganized repair process involving almost all fascicles of the nerve in two diferents segments (neuromas).
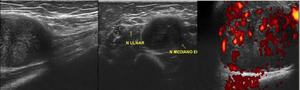
Fig. 32: Ultrasound images (longitudinal and transverse)of median nerve tumor. Doppler shows increased vascularization.
Fig. 33: Ultrasound. Video demonstrates median nerve tumor.
In the majority of patients,
CTS has no obvious cause.
Imaging is not required in the majority of cases of CTS.
However,
imaging plays a role when a secondary cause is suspected,
there is doubt about the diagnosis,
presentation is atypical,
or there are recalcitrant symptoms postoperatively.
Figure 34 llustrates an interdigital neuroma and figure 35 shows a tear of the interdigital nerve (intraoperative photograghs).

Fig. 34: (a) Photograph of a patient´s hand with a soft tissue nodule involving the second digit. (B) and (C) ultrasound images show second finger interdigital radial neuroma.

Fig. 35: Tear of the interdigital nerve caused by a knife wound three days before which resulted in a selective sensitive deficit. Photographs before and after surgical repair. Courtesy of Ayala A, MD Recife, Brazil.



.")
 Coronal STIR and (B) Coronal T1.")
 Coronal and (B) sagittal T2-weighted chest MRI images show soft tissue masses involving brachial plexus bilaterally, the posterior mediastinum an multiple neural foramina. Plexiform neurofibromas in a patient with neurofibromatosis type 1.")
 T1-weighted image. Coronal plane. (B) Diffusion Coronal plane. Nodular hypointense lesion in contact with the upper aspect of the right brachial plexus. Nerve sheath neoplasm.")

 Brachial plexus MRI. 52-year-old man. Coronal T1-weighted image shows soft tissue mass with fat component in the left supraclavicular region (arrow), between the sternocleidomastoid, trapezium and supraspinatus muscles involving the upper trunk of the left brachial plexus. (B) and (C) Intraoperative photographs demonstrate the mass and after its removal respectively.")
 Brachial plexus MRI. Sagittal image shows a heterogeneous soft tissue mass in the left supraclavicular region. Benign neoplasm.(B) Intraoperative photograph of the mass. Courtesy of Souza FH, Hospital da Restauração – Recife-PE, Brazil")



 Coronal T1 weighted image, (B) coronal PD SPIR and (C) sagittal PD SPIR demonstrate a well demarcated lesion involving the distal right ulnar nerve. Nerve sheath tumor.")
and (B) Intraoperative photographs show tumour (schwannoma).
Courtesy of Souza FH, Hospital da Restauração – Recife-PE, Brazil")
 shows normal radial nerve in the forearm. Images (B) and (C) demonstrate hypoechoic fibrous tissue as the result of such a disorganized repair process involving almost all fascicles of the nerve in two diferents segments (neuromas).")
 axial T1 and (B) sagittal PD fat sat.")
 Short axis and (A) long axis ultrsound images of median nerve in the wirst show hypoechoic spots (fascicles) embedded in a hyperechoic epineurium)background.")
 reveals an abrupt change in the size of the nerve at the proximal edge of the retinaculum. The nerve is flattened within the carpal tunnel and markedly swollen proximal to the level of compression (notch sign).
B Long-axis color Doppler US image of the median nerve in the same patient with carpal tunnel syndrome demonstrate flow signals within the median nerve.")

 Ultrasound images. Nerve (N) and M (muscle).")
 located between the radial and ulnar trunks (N) of a bifid median nerve.")
 and short axis (B, C and D) ultrasound images show median nerve and its measurements.")
 and long (A and D) axis ultrasound images show scar (yellow circle in D), posterior interosseous nerve (arrows in A, B and C) and almost all extensor muscles with edema and bruise.")
 and long (B and C) axis ultrasound images show pisotriquetral cyst close to a thickened ulnar nerve (N in A and arrows in C) within Guyon canal. In D short axis images compare hypothenar muscles atrophy and normal muscles on the right.")
 show hypoechoic and thickened ulnar nerve in the forearm. Focal inespecific ulnar neuritis.(C) Contralateral forearm.")


 Median nerve (N), scar tissue involving the median nerve (arrows). (B)Median nerve (N) and cicatricial tissue (cic). (C)Ulnar side, median nerve (N)and cicatricial tissue (arrows).")
of median nerve tumor. Doppler shows increased vascularization.")
 and (B) photographs of the patient´s hand demonstrate atrophy. Ultrasound images (C, D, E, F,and G)show diffuse thickening of upper limb nerves.")

and axial (F, G, H and I)show complete tear of the median nerve, retinaculum and flexor tendons
Intraoperative photographs (D) and (E) before and after repair of median nerve and flexor tendons.Courtesy of Ayala A, MD Recife, Brazil.")