Almost all bone tumors may be found around the knee.
Among benign bone tumors,
between 30 and 35% of chondroblastomas,
50% of osteochondromas and 60% of giant cell tumors affect this region.
A high percentage of nonossifying fibromas is located at the distal end of the femur,
up to 90% in some series.
Aneurysmal bone cysts have a predilection for the proximal tibia.
Of malignant primary bone tumors,
50% of osteosarcomas arise here but only 12–15% of chondrosarcomas.
Plain film radiography,
computed tomography and magnetic resonance imaging are the mainstays of diagnostic imaging for patients with bone tumors.
Certain radiographic patterns,
combined with the age of the patient,
can be very suggestive of specific tumors.
Plain film is the initial modality of choice for detection and assessment the general features of the tumor.
It is the most valuable method to evaluate the radiographic features of the margin between normal bone and a neoplasm (zone of transition),
that is important in distinguishing between benign and malignant bone lesions.
Plain film radiography also demonstrates the extent of cortical destruction,
periosteal reaction,
matrix calcifications and pathological fractures.
Computed tomography scan is particularly useful in evaluating the cortex and matrix and magnetic resonance is determinant to assess the entire extent of the tumor and its relationship to adjacent structures.
- BENIGN BONE TUMORS
Chondroblastoma is a benign bone tumor of cartilaginous origin,
growing from the epiphyseal plate (or some remnant of it).
It is rare,
accounting for less than 1 % of all bone tumors and occurring predominantly in young and male patients (10-20 years of age).
Typically affects the epiphyses and apophyses of long bones.
The most commonly affected site is the femur,
followed be the humerus and tibia.
Malignant transformation has been seen in a small proportion of cases,
associated with local invasion and distant metastases.
Radiography of a chondroblastoma shows well-defined osteolytic epiphyseal lesions,
with a narrow zone of transition,
a reactive sclerotic rim which generally does not break through the cortex and foci of calcification within the lesion (chondroid matrix).
Solid periosteal reaction is seen in up to 50% of cases.
MRI can help diagnostically by showing characteristic changes.
These lesions have signal typical of cartilage,
namely low to intermediate signal in T1 and intermediate to high signal in T2.
Occasionally may be seen fluid-fluid levels presumably due to an associated aneurysmal bone cyst.
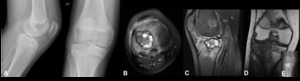
Fig. 1: Chondroblastoma - Plain radiograph (A,E), Magnetic resonance imaging - axial T2FS (B), sagittal T2 FS (C), coronal T1 (D). Radiography shows a well-defined osteolytic epiphyseal lesion, with a narrow zone of transition and a reactive sclerotic rim. It doesn´t break through the cortex and there is no evident chondroid matrix (A). In MRI, the lesion has well defined and lobulated contours, showing a heterogeneous T2 sign with some areas of hypersignal and liquid levels (B,C) that is almost totally isointense in the T1-weighted sequences (D). We also observed perilesional bone edema. In imagem E, we can see the location of the lesion after treatment, which consists of curettage and packing the resulting cavity with bone cement.
Osteochondroma is the most common benign tumor of the skeleton (35% of all benign bone tumors).
It affects young people,
between 10 – 30 years of age,
with no known sex predilection.
This tumor most commonly arise from the appendicular skeleton,
especially around the knee.
The Majority of these tumors are solitary non-hereditary lesions,
but approximately 15% of osteochondromas occur as hereditary multiple exostoses preferably known as hereditary multiple osteochondromas. They can be sessile or pedunculated.
An osteochondroma is composed of normal bone and is covered by cartilage.
There is a continuity of the normal marrow,
cortex,
and periosteum between the exostosis and the host bone.
Osteochondromas grow from their cartilage cap,
which is similar to a growth plate,
and stop growing after skeletal maturation (closure of the growth plate).
Radiographs demonstrate a metaphyseal lesion,
appearing as a sessile or pedunculated osseous mass,
typically growing away from the adjacent joint.
Computed tomography (CT) is helpful in determining the medullary continuity.
Magnetic resonance imaging is the best imaging modality to assess and measure the thickness of the cartilage cap (which assists in predicting the risk of malignant transformation).
The cartilage cap has low to intermediate signal in T1 and high signal in T2.
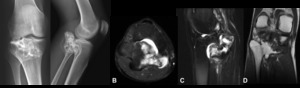
Fig. 2: Osteochondroma - Plain radiograph (A), Magnetic resonance imaging - axial T2FS (B), sagittal T2 FS (C), coronal T1 (D). Radiographs demonstrate a epiphyseal/metaphyseal lesion of the fibula, with typical rings and arcs calcifications (chondroid matrix). In MRI, we observe an exophysial lesion of the proximal fibula, that presents continuity with the bone marrow and has areas of hypersignal in T2, which is compatible with cartilage component. There is a cartilage cap with a thickness of 7 mm.
Enchondromas are relatively common,
accounting for 10–25 % of all benign bone tumors.
The peak incidence is in the third decade and there is no sex predilection sex.
It occurs most commonly in the hands and feet (50%),
but may also involve large tubular bones like femur,
tibia and humerus.
Most patients have no symptoms.
The presence of pain is suspicious for pathological fracture or malignant transformation.
The most common appearance of the enchondroma in radiographs and CT is a geographic lesion with lobulated margins.
The lesion may expand bony margins,
causing cortical thinning.
In large tubular bones,
enchondromas often do not have sclerotic margin and usually contain stippled and curvilinear calcification (cartilaginous matrix).
MRI reveals high signal in T2 and there is no soft tissue mass.
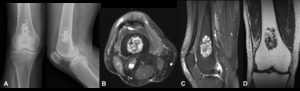
Fig. 3: Enchondroma - Plain radiograph (A), Magnetic resonance imaging - axial T2FS (B), sagittal T2 FS (C), coronal T1 (D). In the distal femoral metaphysis, there is a lesion with stippled and curvilinear calcification (cartilaginous matrix) (A). In MRI, we observe a heterogeneous and multiloculated lesion, with high signal in T2. There is no cortical erosion or soft tissues mass.
Osteoid osteoma is a benign tumor seen in children and young adults (between the ages of 5 and 25 years.
This lesion accounts for approximately 10 % of benign bone tumors,
and usually affects children and adolescents.
There is a male predilection (3:1).
It can occur anywhere in the body but is most commonly located in the cortex of tubular bones,
usually in diaphysis and occasionally in metaphysis of femur and tibia.
Patients experience daily pain that increases at night and tends to be relieved with NSAIDs (such aspirin).
On plain films,
the osteoid osteoma is a small lytic lesion (the nidus),
typically ovoid and measures less than <2 cm of diameter,
surrounded by dense reactive bone formation.
When it is within a joint capsule,
can be associated with marginal sclerosis,
chronic synovitis,
cartilage loss and osteoarthritis.
The best imaging study to demonstrate osteoid osteoma is a CT scan.
Giant cell tumor is a relatively common benign neoplasm,
constituting 5% of primary bone tumors.
It is characterized by the presence of multinucleated giant cells (osteoclast-like cells).
The peak incidence is between the ages of 20 and 45,
being more common in women (2:1).
GCTs typically arise from the metaphysis and adjacent epiphysis,
sometimes with joint involvement.
Malignant transformation has been seen in approximately 5-10% of GCTs.
The typical radiographic appearance of GCT is a lytic geographic lesion with a narrow zone of transition and no marginal sclerosis,
often with mild bone expansion.
In MRI,
the lesion has low to intermediate signal in T1 (solid components enhance) and heterogeneous high signal with areas of low signal intensity in T2 (due to haemosiderin or fibrosis).
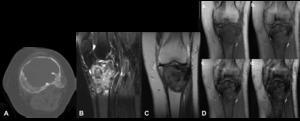
Fig. 4: Giant cell tumour of bone - Non-enhanced computed tomography (bone window) (A), Magnetic resonance imaging - sagittal T2 FS (B), coronal T1 (C), Gradient eco with TE of 4 (a), 9 (b), 14 (c) and 23 (d). In the meta-epiphyseal region, there is a lytic geographic lesion with a narrow zone of transition and no marginal sclerosis, associated with mild bone expansion.
This lesion has hyposignal in T1 and heterogeneous hypersignal in T2FS. In gradient eco sequences it presents areas of hyposignal, more evident with the progressive increase of TE (compatible with hemosiderin deposits).
Nonossifying fibroma is a well circumscribed and solitary fibrous proliferation (called fibrous cortical defect if small).
It is very common in children and adolescents,
with a peak incidence at 10-15 years old (prevalence of 30-40%).
There is a 2:1 male predilection.
They are usually not seen beyond the age of 30,
as they spontaneously heal,
resulting in dense and sclerotic areas in adults.
They originate from the growth plate and are located eccentrically in the metaphysis,
adjacent to the physis,
affecting more commonly the distal femur and tibia.
Nonssoifying fibroma is a wellcircumscribed,
eccentric,
multiloculated osteolytic lesion,
with narrow zone of transition and sclerotic margin,
arising from the cortex.
As the patient get older,
it seems to migrate away from the  growth plate.
MRI appearances are variable,
initially the lesion has high or intermediate T2 signal,
with a peripheral low signal rim corresponding to the sclerotic border.
As it matures and begins to ossify,
the signal becomes low on all sequences.
growth plate.
MRI appearances are variable,
initially the lesion has high or intermediate T2 signal,
with a peripheral low signal rim corresponding to the sclerotic border.
As it matures and begins to ossify,
the signal becomes low on all sequences.
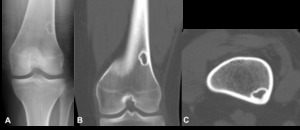
Fig. 5: Non-ossifying fibromas - Plain radiograph (A), Non-enhanced computed tomography (bone window) – sagittal (B), Axial (C). In the cortex of the femur metaphysis, we observe a well circumscribed osteolytic lesion with sclerotic margin. There is no periosteal reaction, matrix or mass of soft tissues.
Aneurysmal bone cyst is a benign lesion consisting of blood-filled cystic cavities.
It is seen mostly in children and adolescents,
between 10–20 years of age.
It occurs in the metaphysis of long bones,
adjacent to an unfused growth plate,
including the proximal tibia and femur.
Aneurismal bone cyst may be primary or secondary to complications of others bone tumors (benign or malignant) that have undergone haemorrhagic cystic change.
Radiographically it presents as an expansible osteolytic lesion with a narrow zone of transition and a fine sclerotic rim (may not be seen on radiographs).
MRI study shows internal septa and characteristic fluid-fluid levels.
The cyst has variable signal,
with surrounding rim of low T1 and T2 signal.
There are focal areas of high T1 and T2 signal representing areas of blood of variable age.
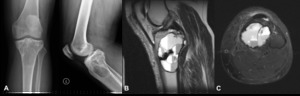
Fig. 6: Aneurysmatic bone cyst. Plain radiograph (A), Magnetic resonance imaging - sagittal T2 weighted (B) and axial T2FS weighted (C). Lytic lesion occupying the proximal epiphyseal and metaphyseal regions of the tibia, with well defined margin and narrow transition zone, without evident periosteal reaction or cortical rupture (A). Cystic lesion located in the proximal epiphyseal and metaphyseal regions of the tibia, with characteristic fluid-fluid levels (B,C).
2.
MALIGNANT BONE TUMORS
Osteosarcoma is a primary malignant mesenchymal tumor in which the neoplastic cells produce osteoid.
It is the second most commons primary bone tumor after multiple myeloma.
The age distribution is bimodal,
with the first peak of incident in the second decade of life (60% of patients under the age of 25) and the second after 50 years of age (secondary to malignant degeneration of others diseases).
There is a slightly male predilection.
The most common sites are the distal femur and proximal tibia.
Most (90 %) arise from the metaphysis of the bone,
but frequently crosses the physeal plate to involve the epiphysis.
The radiologic manifestations of osteosarcoma can vary,
depending on the histological subtype,
although all have features of highly aggressive.
The most common type,
conventional osteosarcoma,
which is intramedullary and high grade,
represents approximately 80% of all osteosarcomas.
It produces osteoid matrix that may range from densely blastic to nearly completely lytic,
with wide zone of transition,
cortical breakthrough,
large soft tissue mass and periosteal reaction.
The telangiectatic osteosarcoma has a geographic bony destruction with wide zone of transition that tends to be more common than permeative bony destruction,
with less osteoid matrix than conventional type.
The parosteal osteosarcoma is a surface lesion the represents the second most common variety of osteosarcoma.
It is a large lobulated exophytic and 'cauliflower-like' mass with central dense ossification adjacent to the bone (the periphery is less mature or even nonossified).
The periosteal osteosarcoma causes a scalloping of the underlying cortex,
although occasionally cortical thickening is seen.
The soft tissue mass extends from the surface of the lesion,
sometimes with spicules of bone emanating in a sunburst pattern.

Fig. 7: High-grade intramedullary osteosarcoma - Plain radiograph (A), Non-enhanced computed tomography (bone window) (B). Osteo-condensing lesion of the distal epiphyseal and metaphyseal regions of the femur, associated with cortical rupture. The lesion presents a voluminous soft tissue mass with typically osteoid mineralization (cloud-like and ill-defined amorphous calcifications).
Chondrosarcoma is a malignant cartilaginous tumor,
that account for 30% of all tumors of the skeletal system.
It can present at any age,
but there is a slightly predilection for older patients and males.
The most common sites are the metaphysis of long bones (namely femur and tibia) and pelvis.
Chondrosarcoma can arise de novo or secondary from an existing benign cartilaginous neoplasm (most often enchondroma).
There are several subtypes of chondrosarcoma,
which vary in terms of location and appearance,
although have some similar general features.
They are large masses at the time of diagnosis,
usually more than 5 cm,
with intralesional calcifications of chondroid matrix (rings and arcs or popcorn calcifications),
endosteal scalloping and cortical breach.
MRI shows a mass of soft tissues with very high intensity in T2 (in non-mineralised portions),
typical of chondroid components.
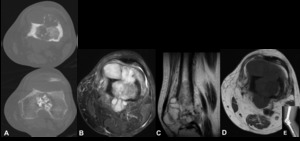
Fig. 8: Chondrosarcoma - Non-enhanced computed tomography (bone window) (A), Magnetic resonance imaging - Axial T2 FS (B), Sagittal T2 (C), Axial T1 (D), Plain radiograph (E). Expansile osteolytic lesion in the distal part of the femur, associated with cortical destruction and soft tissue mass. There is intralesional calcifications of chondroid matrix (rings and arcs or popcorn calcifications). MRI shows a heterogeneous hyposignal in T1 and hypersignal in T2, with some hypointense punctiform areas translating foci of calcification. In image E, we can see the same patient after the surgery, with bone resection and replacement with metallic prosthesis.
Ewing sarcoma is the second most common highly malignant primary bone tumor of childhood,
arising in the bone marrow,
without any matrix production.
Typically affects patients younger than 20 years (80%) and has a slight male predilection (2:1).
It occurs most frequently in the diaphysis or meta-diaphyseal portion of long bones,
namely of the femur,
and its location around the knee accounts for approximately 10% of the cases.
The Ewing sarcoma appears as an large and ill defined osteolytic lesion,
associated with permeative pattern.
It is often associated with “onion-skin” multilayered periosteal reaction.
A large and ill defined soft tissue mass is a frequent association in Ewing tumor,
often without foci of calcification.
MRI is essential to elucidate the soft tissue involvement.
The lesion has low to intermediate signal in T1 and heterogeneously high signal in T2.
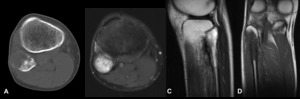
Fig. 9: Ewing Sarcoma - Non-enhanced computed tomography (bone window) (A), Magnetic resonance imaging - Axial T2 FS (B), Sagittal T2 (C), Coronal T1 (D). Osteolytic lesion of the proximal part of the fibula, with cortical rupture and periosteal reaction (A). It has hyposignal in T1 and hypersignal in T2. There is no evidence of soft tissue mass (B,C,D).
Multiple myeloma is the most common primary malignant bone neoplasm in adults.
Most cases occur in patients in the fifth or sixth decade of life,
with male predilection (2:1).
Its distribution is according the presence of red marrow,
thus is mostly encountered in the axial skeleton and proximal appendicular skeleton,
including long bones (namely femur).
The radiologic findings in multiple myeloma can be variable,
being the most common appearances a diffuse osteopenia pattern and osteolytic lesions with the typical punched-out aspect,
endosteal scalloping,
broad zone of transition and no periosteal reaction.
Plasmacytoma is a tumor that is histologically identical to multiple myeloma,
although it is a single expansile lesion,
mostly seen in vertebrae and pelvis.
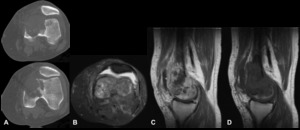
Fig. 10: Plasmacytoma - Non-enhanced computed tomography (bone window) (A), Magnetic resonance imaging - Axial T2 FS (B), Sagittal T1 (C), Sagittal T1 after contraste injection (D). In the distal part of the left femur, there is an osteolytic lesion that causes bone destruction, with signs of cortical rupture. In MRI, the lesion is hypointense in T1 and hyperintense in T2. It has a very heterogeneous matrix, predominantly solid. After administration of gadolinium, it undergoes heterogeneous enhancement, with some central hypointense areas, compatible with areas of necrosis. There is a moderate joint effusion.
Skeletal metastases are the most common malignant tumors of bone,
accounting for 70%.
Cancers that most frequently spread to bone include; breast,
lung,
thyroid,
kidney,
and prostate.
Metastases are most commonly localized according the distribution of red marrow,
namely in the axial skeleton and proximal femur and humerus.
Metastases around the knee are uncommon.
The metastases may have different types of presentation,
like an osteolytic,
osteoblastic or mixed pattern,
depending the primary tumor.
Typically,
there is no periosteal reaction associated with bone metastases.
MRI is important to assess the entire extent of the tumor and its relationship to adjacent structures.
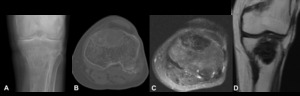
Fig. 11: Metastasis from breast tumor- Plain radiograph (A), Non-enhanced computed tomography (bone window) (B), Magnetic resonance imaging - Axial T2 FS (C), Sagittal T1 (D). Intramedullary osteolytic lesion located in the epiphysis of the tibia, with signs of cortical invasion. It has hyposignal in T1 and T2. There is no soft tissue masses.

, Magnetic resonance imaging - axial T2FS (B), sagittal T2 FS (C), coronal T1 (D). Radiography shows a well-defined osteolytic epiphyseal lesion, with a narrow zone of transition and a reactive sclerotic rim. It doesn´t break through the cortex and there is no evident chondroid matrix (A). In MRI, the lesion has well defined and lobulated contours, showing a heterogeneous T2 sign with some areas of hypersignal and liquid levels (B,C) that is almost totally isointense in the T1-weighted sequences (D). We also observed perilesional bone edema. In imagem E, we can see the location of the lesion after treatment, which consists of curettage and packing the resulting cavity with bone cement.")
, Magnetic resonance imaging - axial T2FS (B), sagittal T2 FS (C), coronal T1 (D). Radiographs demonstrate a epiphyseal/metaphyseal lesion of the fibula, with typical rings and arcs calcifications (chondroid matrix). In MRI, we observe an exophysial lesion of the proximal fibula, that presents continuity with the bone marrow and has areas of hypersignal in T2, which is compatible with cartilage component. There is a cartilage cap with a thickness of 7 mm.")
, Magnetic resonance imaging - axial T2FS (B), sagittal T2 FS (C), coronal T1 (D). In the distal femoral metaphysis, there is a lesion with stippled and curvilinear calcification (cartilaginous matrix) (A). In MRI, we observe a heterogeneous and multiloculated lesion, with high signal in T2. There is no cortical erosion or soft tissues mass.")
 (A), Magnetic resonance imaging - sagittal T2 FS (B), coronal T1 (C), Gradient eco with TE of 4 (a), 9 (b), 14 (c) and 23 (d). In the meta-epiphyseal region, there is a lytic geographic lesion with a narrow zone of transition and no marginal sclerosis, associated with mild bone expansion.
This lesion has hyposignal in T1 and heterogeneous hypersignal in T2FS. In gradient eco sequences it presents areas of hyposignal, more evident with the progressive increase of TE (compatible with hemosiderin deposits).")
, Non-enhanced computed tomography (bone window) – sagittal (B), Axial (C). In the cortex of the femur metaphysis, we observe a well circumscribed osteolytic lesion with sclerotic margin. There is no periosteal reaction, matrix or mass of soft tissues.")
, Magnetic resonance imaging - sagittal T2 weighted (B) and axial T2FS weighted (C). Lytic lesion occupying the proximal epiphyseal and metaphyseal regions of the tibia, with well defined margin and narrow transition zone, without evident periosteal reaction or cortical rupture (A). Cystic lesion located in the proximal epiphyseal and metaphyseal regions of the tibia, with characteristic fluid-fluid levels (B,C).")
, Non-enhanced computed tomography (bone window) (B). Osteo-condensing lesion of the distal epiphyseal and metaphyseal regions of the femur, associated with cortical rupture. The lesion presents a voluminous soft tissue mass with typically osteoid mineralization (cloud-like and ill-defined amorphous calcifications).")
 (A), Magnetic resonance imaging - Axial T2 FS (B), Sagittal T2 (C), Axial T1 (D), Plain radiograph (E). Expansile osteolytic lesion in the distal part of the femur, associated with cortical destruction and soft tissue mass. There is intralesional calcifications of chondroid matrix (rings and arcs or popcorn calcifications). MRI shows a heterogeneous hyposignal in T1 and hypersignal in T2, with some hypointense punctiform areas translating foci of calcification. In image E, we can see the same patient after the surgery, with bone resection and replacement with metallic prosthesis.")
 (A), Magnetic resonance imaging - Axial T2 FS (B), Sagittal T2 (C), Coronal T1 (D). Osteolytic lesion of the proximal part of the fibula, with cortical rupture and periosteal reaction (A). It has hyposignal in T1 and hypersignal in T2. There is no evidence of soft tissue mass (B,C,D).")
 (A), Magnetic resonance imaging - Axial T2 FS (B), Sagittal T1 (C), Sagittal T1 after contraste injection (D). In the distal part of the left femur, there is an osteolytic lesion that causes bone destruction, with signs of cortical rupture. In MRI, the lesion is hypointense in T1 and hyperintense in T2. It has a very heterogeneous matrix, predominantly solid. After administration of gadolinium, it undergoes heterogeneous enhancement, with some central hypointense areas, compatible with areas of necrosis. There is a moderate joint effusion.")
, Non-enhanced computed tomography (bone window) (B), Magnetic resonance imaging - Axial T2 FS (C), Sagittal T1 (D). Intramedullary osteolytic lesion located in the epiphysis of the tibia, with signs of cortical invasion. It has hyposignal in T1 and T2. There is no soft tissue masses.")