Pathogenesis
Generally one may distinguish three clinical stages (acute,
subacute and chronic),
although there may be some overlap.
Acute osteomyelitis is typical of children,
has a rapid onset and may present with systemic toxicity.
The bones most commonly affected are the tibia,
the femur,
and the humerus.
Although it is relatively uncommon in healthy adults,
it can occur in immunocompromised individuals or intravenous drug abusers.
The subacute stage or Bodie’s abscess is more insidious and can be due to inadequate treatment or low virulence of the organisms.
It usually presents with indolent pain and there may be effusion in the adjacent joint and some atrophy of the muscles.
The most common location is the knee and the ankle,
frequently in adolescent boys.
Chronic OM generally presents as recurrent episodes of acute inflammation over a period of more than 6 years to many years.
There may be a discharging sinus and there is usually a history of previous acute OM,
trauma or orthopedic implants that was complicated by infection.
The routes of contaminations may vary according to age.
In children,
the hematogenous spread is the predominant route of infection,
whereas in adults spread from a contiguous source,
direct contamination or post-operative infection is much more frequent. Staphylococcus aureus is the causative organism in up to 80% of cases. Haemophilus influenzae and group B streptococcus are common causative agents in children,
while gram-negative bacteria can be found in adult and diabetic cases.
The nature of blood supply to the diaphysis,
metaphysis and epiphysis depends on the age of the patient.
In infants younger than 18 months,
there are metaphyseal and transphyseal blood vessels,
allowing both metaphyseal and epiphyseal origin of infection.
In children between 18 months and 16 years,
the epiphysis has its own nutrient vessels (veins and arteries) whilst the metaphysis and diaphysis share the same vessels.
The physis creates a natural barrier,
preventing the spread of osteomyelitis in the epiphysis and joints.
After the closure of the growth plate,
there is once again restoration of the transphyseal vascularization,
which may cause potential epiphyseal spread of infection (Fig.
1).

Fig. 1: Vascularization of the long bone according to age, modified from Desimpel (1). (A) In infants younger than 18 months, there are transphyseal blood vessels, allowing both metaphyseal and epiphyseal origin of infection. (B) In children between 18 months and 16 years, the physis creates a natural barrier, preventing spread of osteomyelitis in the epiphysis and joints. (C) After closure of the growth plate, there is restoration of the transphyseal vascularization, which may cause potential epiphyseal spread of infection.
In OM secondary to hematogenous spread or direct inoculation,
bacterial proliferation within the bone inducing an acute suppurative response,
with the accumulation of pus within the medullary cavity.
This leads to an increase in intramedullary pressure and vascular congestion.
Reactive bone and granulation tissue may form around the pus,
giving rise to a well-circumscribed intra-osseous abscess,
also known as a Brodie’s abscess.
The rise in intramedullary pressure may lead to rupture of the bony cortex,
producing a cortical defect,
the cloaca.
The intramedullary pus can then spread outward through the cloaca and form a subperiosteal abscess,
with an elevation of the periosteum and disruption the periosteal blood supply to the bone.
Accumulation of subperiosteal pus leads to rupture of the periosteum and spread of infection to soft tissues through a sinus tract.
Subperiosteal abscesses are more common in children,
as the cortical bone is thinner and more easily ruptured and the periosteum is also more loosely attached to the surface of the cortex and is easily separated (Fig.
2).
If the acute infection is inadequately treated,
there will be progression to chronic osteomyelitis.
There is osteonecrosis due to disruption of the intraosseous and periosteal blood supply and a fragment of dead infected bone becomes separated - the sequestrum.
The bacteria within the sequestrum are protected from antibiotics and the immune response,
forming a nidus for chronic infection (Fig.
2).

Fig. 2: The pathogenesis of osteomyelitis, modified from Lee (4). In acute OM, a collection of pus is surrounded by granulation tissue and reactive bone, forming an intraosseous abscess. Due to raised intramedullary pressure, there may be rupture of the cortex, creating a defect (the cloaca), which allows drainage to the surrounding tissures, forming either a subperiosteal abscess or a soft tissue abscess. In chronic OM, there is disruption of the intraosseous and periosteal blood supply, leading to osteonecrosis and the formation of a necrotic bone fragment (the sequestrum). This sequestrum is surrounded by a reactive shell of new bone, known as an involucrum. There may be a sinus tract, draining pus from bone to the skin surgace, both in acute and chronic osteomyelitis.
Imaging Findings
Conventional radiography
Plain radiography has low sensitivity and specificity for detecting acute osteomyelitis.
Radiographic changes of acute osteomyelitis may lag behind by 10 to 14 days,
as there must be the destruction of more than 60% of trabecular bone before OM can be detected.
Therefore,
as many as 80% of patients will have a normal radiograph in the first two weeks.
Nevertheless,
a baseline radiograph is fundamental,
as it not only excludes other causes,
but it also serves as a means of assessing progress after treatment.
The earliest sign observed may be effacement of fat planes with diffuse soft tissue swelling.
After 10 days,
there may be seen a periosteal reaction secondary to an elevation of the periosteum or a well-circumscribed bony lucency representing an intraosseous abscess.
However,
these findings are nonspecific and can also be seen in stress fractures,
bone tumors or soft tissue infections.
In the subacute phase,
usually there is a lucent lesion in the epiphysis or the metaphysis,
which can be associated with a linear track.
Periosteal reactions may be subtle or even absent (Fig.
3).

Fig. 3: Acute/subacute osteomyelitis in an 11-year-old girl. Conventional radiography of the knees shows lucent lesions on the right tibial metaphysis abuting the physis.
In chronic OM,
there is extensive bony remodeling,
with marked cortical destruction,
a disorganized trabecular pattern and ill-defined bony lucencies.
A sequestrum may be visible as a focal sclerotic lesion with a lucent rim.
However,
these findings are better illustrated with computed tomography (CT) (Fig.
4).
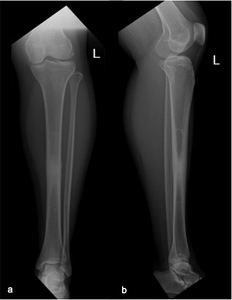
Fig. 4: Chronic osteomyelitis in a 42-year-old woman. Conventional radiography of the left leg on anteroposterior (a) and lateral incidence (b) showing a sclerotic alteration of the tibial diaphysis with periosteal reaction.
Ultrasound
Ultrasonography (US) has a complementary role in the investigation of osteomyelitis.
It allows easy comparison of both sides and is an accurate and quick tool to detect subperiosteal spread in acute OM,
particularly in children because of loose attachment of the periosteum.
This may be particularly useful when plain radiographs are normal.
Nevertheless,
the absence of this sign does not exclude the disease (Fig.
5)

Fig. 5: Acute osteomyelitis in a 4-year-old girl. Ultrasound shows a periosteal collection involving the anterior surface of the radius, accompanied by thickening and hyperechogenicity of the muscle, due to edema.
The US may also depict soft tissue abscesses and the presence of joint effusion.
A soft tissue abscess appears as a hypoechogenic collection to normal muscle with a peripheral vascularized rim of increased Power Doppler signal.
It also allows guided aspiration and/or biopsy.
It can also have a particularly valuable role in the assessment of other causes of soft tissue swelling and pain,
such as cellulitis,
thrombophlebitis,
bursitis,
hematoma,
tenosynovitis or subcutaneous abscess.
Computed tomography
CT is useful in the detection of early bone destruction or the presence of small sequestrum (Fig.
6,
7).
Soft tissue or marrow abscesses may demonstrate rim enhancement after contrast agent administration.
Gas within the infected bone is considered to be the earliest sign seen on CT.
It may provide information regarding the presence of cloaca,
cortical destruction and the thickness of the involucrum.
Particularly in the assessment of sequestrum formation,
CT is more accurate than plain radiography and MRI (Fig.
7).
In chronic OM it can depict the extensive bony remodeling,
with marked cortical destruction,
disorganized trabecular pattern and ill-defined bony lucencies (Fig.
7,
8).
CT also enables precise localization for biopsy and aspirations of infected bone or abscesses.
However,
due to radiation dose,
use of CT should be carefully outweighed in children.

Fig. 6: Acute osteomyelitis in a 46-year-old male. Sagittal CT shows focal bony lysis and cortical irregularities. There is no evidence of a sequestrum.

Fig. 7: Chronic osteomyelitis in a 33-year-old woman. Coronal CT (a, b) show marked bone remodeling with cortical thickening. There is an intramedular linear image consistent with a sequestrum (b, c) and there is drainage through a fistula tract (a).

Fig. 8: Chronic osteomyelitis in a 42-year-old woman. Axial (A) and sagittal CT (B) depicting extensive bony remodeling with diffuse cortical thickening.
Magnetic resonance imaging
Magnetic Resonance Imaging (MRI) is the modality of choice for early detection of acute OM.
It is highly sensitive (approaching 100%),
showing changes as early as 3 to 5 days after the onset of infection.
It offers excellent anatomical detail,
allowing assessment of the extent of involvement and the activity of the disease.
MRI is also effective in monitoring treatment,
especially in subacute and chronic osteomyelitis,
and helps the surgeon to plan the optimal surgical management and to assess the extent of devitalized tissue.
The typical sequences included in the evaluation of OM include:
- T1-weighted (T1W) sequences for anatomical detail,
delineation of the medulla,
cortex,
periosteum and soft tissues.
Fluid has low signal,
abscesses have low to intermediate signal and fat has a high signal.
- Fluid-sensitive sequences include T2-weighted (T2W),
fat-suppressed (FS) and short-tau inversion recovery (STIR) sequences.
They are useful for detecting infection and inflammation,
which cause an increase in tissue fluid content and a high signal.
In fat-suppressed and STIR sequences,
the signal from fat is decreased,
increasing the visibility of inflammatory changes and fluid collections.
- Proton density-weighted (PD) sequences are intermediately weighted between T1 and T2.
They provide good anatomical detail but with less tissue contrast compared to T1W images.
- FS-T1 sequences with gadolinium may also be useful.
If a possible abscess or sinus tract is seen,
post-contrast FS-T1 sequences will allow further characterization.
In epiphyseal infection,
it is essential,
as the unenhanced images may appear normal.
Contrast administration is also fundamental for differentiating an abscess from a phlegmon.
Acute and Subacute Osteomyelitis
Bone marrow edema is the earliest feature seen on MRI and can be detected within three to five days after disease onset.
As the marrow becomes congested with fluid and pus,
it loses its high T1 signal from fat and changes to a low signal on T1W and high signal on fluid-sensitive sequences.
The abnormal marrow will enhance after gadolinium administration (Fig.
9).

Fig. 9: Acute osteomyelitis in a 14-year-old boy. Axial T1 FS after the administration of intravenous contrast shows diffuse bone marrow edema with inflammatory changes also involving the adjacent muscles.
Intraosseous and subperiosteal abscesses will have low signal on T1W images and high signal on fluid-sensitive sequences,
with a thin rim of intermediate T1 signal seen surrounding the abscess,
representing hypervascular granulation tissue.
On post-contrast FS-T1 images,
this peripheral granulation tissue will enhance while the central pus-filled cavity remains low in signal intensity (Fig.
10,
11,
12).
This pattern of peripheral enhancement is known as the penumbra sign and can help differentiate an abscess from a phlegmon,
which has a more heterogeneous enhancement.
The cloaca can be seen in both acute and chronic osteomyelitis as a cortical defect draining pus from within the medulla to the surrounding soft tissues.
It is most easily seen on fluid-sensitive sequences because it will have a high signal (Fig.
11).

Fig. 10: Acute osteomyelitis in an 11-year-old female. Axial T1 FS before (a) and after the administration of intravenous contrast (b) show diffuse edema of the tibial metaphysis with a small heterogeneous collection limited by a sclerotic rim. There are also inflammatory changes involving the popliteus muscle and tendon (b).

Fig. 11: Acute osteomyelitis in a 58-year-old male. Sagital (a) and axial (b) T1 FS after the administration of intravenous contrast show a nonenhancing intraosseous abscess with peripheral enhancement and drainage to the subcutaneous tissue through a cloaca (b).

Fig. 12: Acute osteomyelitis in a 46-year-old male. Sagittal DP FS (a), sagittal T1 (b) and axial T1 FS after the administration of intravenous contrast (c) depict marked signal change of the calcaneus, with cortical destruction, intraosseous liquid collection and extensive bone marrow changes. These changes also involve the cuboid and there are also extensive signs of cellulitis and myositis.
The sinus tract is seen as a linear fluid-filled structure extending from bone to the skin surface,
also lined by hypervascular granulation tissue.
There may be also periostitis,
seen as an elevation of the low-signal periosteum off the cortical surface.
Chronic Osteomyelitis
The sequestrum can be difficult to depict on MRI.
It appears dark on all sequences as it is a fragment of necrotic bone.
After administration of gadolineum,
enhancement of infected marrow is seen,
as it has hypervascular granulation tissue,
but the sequestrum never enhances (Fig.
13).
The involucrum appears as a thickened shell of bone around the sequestrum,
with either normal signal or edema (Fig.
14).

Fig. 13: Chronic osteomyelitis in a 33-year-old woman. Axial T1 FS after the administration of intravenous contrast shows marked cortical thickening with a nonenhancing intramedular linear image consistent with a sequestrum (a). There is drainage through a fistula tract (b).

Fig. 14: Chronic osteomyelitis in a 42-year-old woman. Axial T1 FS before (a) and after the administration of intravenous contrast (b) show diffuse cortical thickening of the tibial diaphysis with regular periosteal reaction and bone marrow edema enhancing after intravenous contrast. There are no images of sequestrum or abscesses.

. (A) In infants younger than 18 months, there are transphyseal blood vessels, allowing both metaphyseal and epiphyseal origin of infection. (B) In children between 18 months and 16 years, the physis creates a natural barrier, preventing spread of osteomyelitis in the epiphysis and joints. (C) After closure of the growth plate, there is restoration of the transphyseal vascularization, which may cause potential epiphyseal spread of infection.")
. In acute OM, a collection of pus is surrounded by granulation tissue and reactive bone, forming an intraosseous abscess. Due to raised intramedullary pressure, there may be rupture of the cortex, creating a defect (the cloaca), which allows drainage to the surrounding tissures, forming either a subperiosteal abscess or a soft tissue abscess. In chronic OM, there is disruption of the intraosseous and periosteal blood supply, leading to osteonecrosis and the formation of a necrotic bone fragment (the sequestrum). This sequestrum is surrounded by a reactive shell of new bone, known as an involucrum. There may be a sinus tract, draining pus from bone to the skin surgace, both in acute and chronic osteomyelitis.")

 and lateral incidence (b) showing a sclerotic alteration of the tibial diaphysis with periosteal reaction.")


 show marked bone remodeling with cortical thickening. There is an intramedular linear image consistent with a sequestrum (b, c) and there is drainage through a fistula tract (a).")
 and sagittal CT (B) depicting extensive bony remodeling with diffuse cortical thickening.")
 and after the administration of intravenous contrast (b) show diffuse edema of the tibial metaphysis with a small heterogeneous collection limited by a sclerotic rim. There are also inflammatory changes involving the popliteus muscle and tendon (b).")
 and axial (b) T1 FS after the administration of intravenous contrast show a nonenhancing intraosseous abscess with peripheral enhancement and drainage to the subcutaneous tissue through a cloaca (b).")
, sagittal T1 (b) and axial T1 FS after the administration of intravenous contrast (c) depict marked signal change of the calcaneus, with cortical destruction, intraosseous liquid collection and extensive bone marrow changes. These changes also involve the cuboid and there are also extensive signs of cellulitis and myositis.")

. There is drainage through a fistula tract (b).")
 and after the administration of intravenous contrast (b) show diffuse cortical thickening of the tibial diaphysis with regular periosteal reaction and bone marrow edema enhancing after intravenous contrast. There are no images of sequestrum or abscesses.")