We reviewed MRI studies performed at our institution,
during the initial evaluation of patients with a diagnosis of STS of the extremities,
to illustrate findings relevant for surgical planning,
such as tumour size,
location,
depth extension,
peritumoral oedema,
neurovascular and bone/joint invasion.
STS commonly present as an enlarging,
painless mass.
Distant metastatic disease is uncommon,
being more frequent in large,
deep and high-grade tumours.
Initial evaluation of a soft tissue mass encompasses clinical history,
physical examination,
imaging,
and histologic evaluation through biopsy.
STS patient should be referred to specialized centres,
with major therapeutic goals including survival improvement,
avoidance of local recurrence,
maximizing function and minimizing morbidity. Treatment usually encompasses surgery and/or radiotherapy, with isolated excision typically reserved for small (<5 cm),
low-grade and superficial tumours.
Imaging plays a crucial role in preoperative planning,
helping prevent inadequate incisions,
incomplete resections as well as damage to adjacent neurovascular structures. Diagnostic imaging should be performed before the biopsy,
to avoid soft tissue oedema and haemorrhage that may interfere with the evaluation of the lesion.
Some studies have found no significant difference between CT and MRI in determining tumour involvement of muscle,
bone,
joints or neurovascular structures. Nevertheless, MRI is the main imaging modality used due to its superior soft tissue resolution.
Distant disease evaluation is usually performed using chest CT,
complemented by abdominal and pelvic CT in round cell/myxoid liposarcomas and brain CT in angiosarcoma and alveolar soft part sarcomas.
PET-CT has been reported to be a useful tool for determining patient prognosis and tumour grade and treatment response,
but it is still not routinely used in a clinical setting.
The most widely use overall staging system is from the AJCC/TNM staging system (8thedition,
2017).
Although this system only classifies the tumour according to its greatest dimension (Fig. 1),
other key findings are important for determining the patient prognosis and therapeutic planning,
such as location,
neurovascular involvement,
bone invasion and the peritumoral zone.
| T1 |
≤5cm
|
| T2 |
>5 and ≤10cm |
| T3 |
>10cm and ≤15cm |
| T4 |
>15cm |
| N0 |
No/unknown regional lymph nodes metastasis |
| N1 |
Regional lymph node metastasis |
| M0 |
No distant metastasis |
| M1 |
Distant metastasis |
Table 1 - AJCC/TNM staging system (8thedition,
2017) for the evaluation of STS of the extremities.

Fig. 1: The greatest dimension of the tumor is used to classify the T stage according to the AJCC/TNM staging system (8th edition, 2017). A - Pleomorphic sarcoma with 4,8cm (T1). B - Myxofibrosarcoma with 8cm (T2). C - Rhabdomyosarcoma with 18,5cm (T4).
LOCATION
STS typically grow along tissue planes,
rarely crossing major fascial planes or bones. Tumour location should be determined,
namely if it is superficial or deep relating to the deep fascia (Fig. 2).
If it is deep,
the compartments involved should be identified (Fig. 3).
Both the arm and upper are divided in two compartments (anterior and posterior),
while the thigh is divided in three (anterior,
posterior and medial) and the leg in four (anterior,
lateral,
superficial posterior and deep posterior).
Some tumours have borders that are less defined and should be referred to as extra-compartmental (eg.
popliteal fossa).
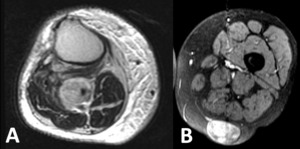
Fig. 2: STS should be classified as deep (A) or superficial (B) in relation to the deep fascia.
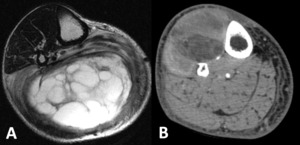
Fig. 3: A- Rhabdomyosarcoma affecting the superficial posterior and deep posterior compartments of the left leg demonstrated in a T2 axial image. The fat plane between the tumor and the neurovascular bundle is preserved. B - Liposarcoma affecting the anterior and lateral compartments of the right leg demonstrated in CT. There is loss of the normal fat plane between the tumor and the neurovascular bundle, and invasion should be considered.
NEUROVASCULAR INVOLVEMENT
Neurovascular bundle involvement should be considered when there is loss of the normal fat plane between the tumour and the neurovascular structures,
with encasement being defined as an abutment superior to 180º (Fig. 4).
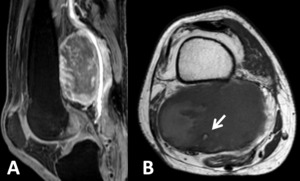
Fig. 4: Rhabdomyosarcoma in the right popliteal fossa demonstrated in sagittal T1FS Gd+ (A) and axial T1 weighted images (B). There is encasement of the neurovascular bundle, with the lesion surrounding the popliteal vessels (arrow).
BONE INVASION
Bone invasion has been correlated with a higher frequency of disease-related mortality and can be identified on CT (Fig. 5) or MRI.
Typical findings in the latter include changes on the cortical and medullary bone signal intensity.
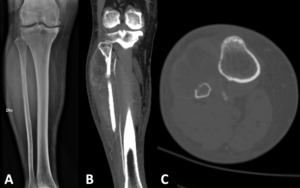
Fig. 5: Large liposarcoma in the anterior and lateral compartments of the right leg. There is an invasion of the diaphysis of the fibula, which has a heterogeneous pattern in the radiograph (A), with the CT images in the coronal (B) and axial (C) planes, best depicting the cortical disruption.
PERITUMORAL ZONE
STS grow centrifugally,
compressing the surrounding tissue and thus creating a pseudo-capsule.
The peritumoral zone should be carefully evaluated to identify oedema,
characterized by an increased signal intensity in T2 weighted-images (Fig. 6).
Peritumoral oedema is associated with high-grade tumours and should be included in the surgical resection margins and radiotherapy planning as it though to represent areas of neovascularization and satellite lesions.
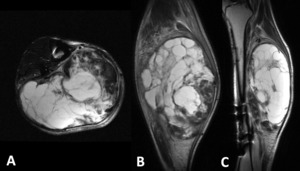
Fig. 6: Rhabdomyosarcoma of the right leg affecting the superficial posterior and deep posterior compartments. demonstrated in T2 weighted images in the axial (A), coronal (B) and sagittal (C) planes. The peritumoral zone shows a diffuse increase in signal intensity, reflecting the presence of peritumoral edema, best depicted here in the coronal and sagittal planes.

. A - Pleomorphic sarcoma with 4,8cm (T1). B - Myxofibrosarcoma with 8cm (T2). C - Rhabdomyosarcoma with 18,5cm (T4).")
 or superficial (B) in relation to the deep fascia.")

 and axial T1 weighted images (B). There is encasement of the neurovascular bundle, with the lesion surrounding the popliteal vessels (arrow).")
, with the CT images in the coronal (B) and axial (C) planes, best depicting the cortical disruption.")
, coronal (B) and sagittal (C) planes. The peritumoral zone shows a diffuse increase in signal intensity, reflecting the presence of peritumoral edema, best depicted here in the coronal and sagittal planes.")