ESSR 2019 / P-0146
MRI imaging of a rare complication: Partial entwinement and splitting of sciatic nerve following closed reduction of a dislocated revised hip prosthesis
Congress:
ESSR 2019
Poster Number:
P-0146
Type:
Educational Poster
Keywords:
Prostheses, Image verification, Acute, Surgery, Imaging sequences, Complications, MR, Image manipulation / Reconstruction, Conventional radiography, Neuroradiology peripheral nerve, Musculoskeletal system, Anatomy
Authors:
C. Y. Ng1, J. S. Wong2, P. Suresh1, J. Keenan1; 1Plymouth/UK, 2Oswestry/UK
DOI:
10.26044/essr2019/P-0146

Fig. 1:
AP and lateral plain radiographs demonstrating the posteriorly dislocated left...
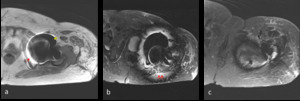
 signal void (yellow arrow) and signal pile-up (red arrow) (b) failure of adjacent fat suppression on STIR sequence (red arrow) (c) peri-prosthetic geometric distortion.")
Fig. 2:
Non metal-artifact suppression MRI demonstrating peri-prosthetic artifacts: (a)...
 as reflected by it's positional plane adjacent to the left lesser trochanter.")
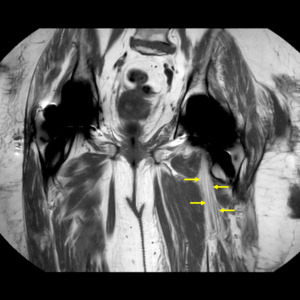
Fig. 3:
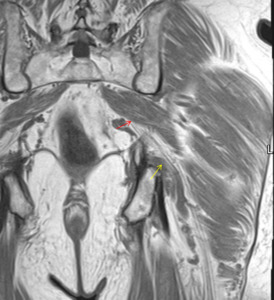
Coronal T1-weighted MARS, demonstrating the anteriorly displaced left sciatic...
 exiting the greater sciatic foramen in a relatively horizontal and anterior course compared to the right side. This reflects the tension the nerve is subjected to by the entwinement.")
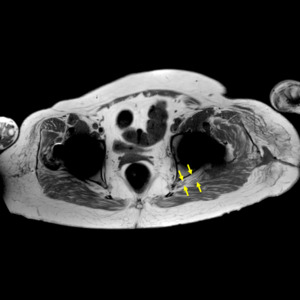
Fig. 4:
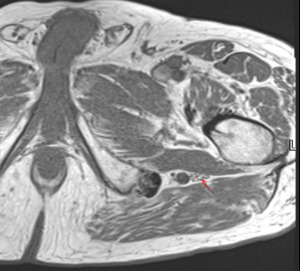
Axial T1-weighted MARS demonstrating the left sciatic nerve (yellow arrows)...
 at the level of the inferior border of the left prosthetic femoral neck, demonstrating an anteriorly displaced nerve bundle (blue arrow) emerging medial to the metal artifact.
(b) A posterior nerve bundle (yellow arrows) is shown to course anteriorly to rejoin the thicker anterior bundle. The posterior femoral cutaneous nerve (white arrow) is identified.")
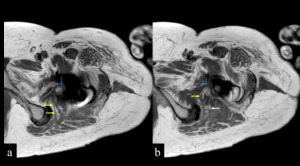
Fig. 5:
Axial T1w MARS - (a) at the level of the inferior border of the left prosthetic...

Fig. 6:
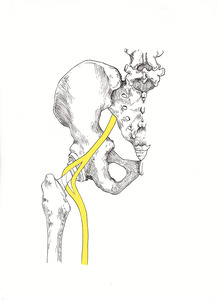
Illustrative diagram by Caryn Koh - Posterior view of the left hip...
 exiting the greater sciatic foramen anterior to the piriformis muscle (yellow arrow).")
Fig. 7:
Axial T1w MRI of the left hip - demonstrating the left sciatic nerve (red...
 crossing the superior border of the superior gemellus muscle posteriorly (yellow arrow) and just passing the inferior border of the piriformis muscle (green arrow).")
Fig. 8:
Axial T1w MRI of the left hip - demonstrating the left sciatic nerve (red...
 and coursing over the superior gemellus muscle (yellow arrow) posteriorly.")
Fig. 9:
Coronal T1w MRI of the left hip - demonstrating the left sciatic nerve passing...

Fig. 10:
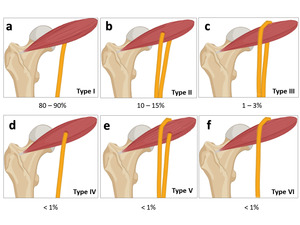
Illustrative diagram - demonstrating the classification of the variants of the...
 as one bundle at the level of the ischial tuberosity.")
Fig. 11:
Axial T1w MRI of the left hip - demonstrating a Type I left sciatic nerve (red...