Introduction
CPPD is an umbrella term used for all instances of calcium pyrophosphate (CPP) crystal deposition,
as proposed by the EULAR (European League Against Rheumatism) CPPD Task Force.
Clinical presentations of CPPD include (table 1):
-
asymptomatic CPPD
-
OA with CPPD (osteoarthritis with CPPD)
-
acute CPP crystal arthritis
-
chronic CPP crystal inflammatory
CPPD occurs most frequently in articular,
hyaline or fibro-cartilage; less frequently,
it can affect tendons and joint capsule structures.
This form of crystal deposition is well documented and commonly described as:
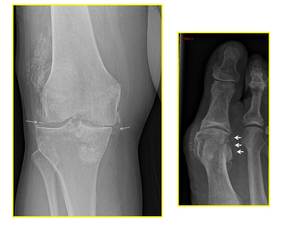
Fig. 1: XR Knee - AP view (left): chondrocalcinosis of the menisci (white arrows) and osteoarthritis.
XR Toes - AP view (right): peri-articular/capsular calcification (white arrows).

Fig. 2: XR Wrist (left) - AP view: chondrocalcinosis at the TFCC (white circle).
XR Hand (right) - AP view: articular calcifications at the MCPJ in the same patient.
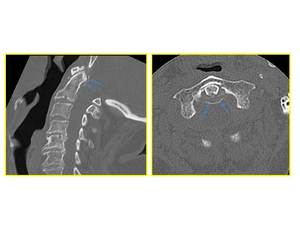
Fig. 3: Sagittal (left) and axial (right) CT images: focal high attenuation material around the odontoid process.
Documented risk factors for CPP disease are:
- age
- osteoarthritis
- several metabolic conditions (hyperparathyroidism,
hemochromatosis,
hypophosphatemia,
hypomagnesemia and gout).
This condition is rare under the age of 50 and a familiar or metabolic predisposition should be suspected in CPPD presenting under the age of 45.
Prevalence reported shifts between 2 % and 8.5%; the highest being in the knees,
followed by the wrist and hands but this estimate is based largely on radiographically detected chondrocalcinosis (CC).
In asymptomatic patients,
these calcifications visible on imaging are an incidental finding and no treatment is necessary.
CPP deposition can,
however,
induce acute arthritis and represents the third most common inflammatory arthritis.
Acute attacks of CPP disease can also occur in the context of acute illness (eg infection),
joint trauma or in the postoperative period,
particularly after parathyroidectomy or hip-fracture repair.
Although imaging might assist with the diagnosis of CPPD,
the EULAR recommends identifications of crystal on synovial fluid or occasionally on biopsies tissue for a definite diagnosis. Moreover,
radiographic chondrocalcinosis might support the diagnosis but its absence does not exclude it.
Axial deposition
Axial or spinal CPP deposition,
in the form of soft tissue calcification,
is more commonly found in the cervical spine.
It can occur at the atlanto-axial junction,
in the intervertebral disc,
in the facet joints and spinal ligaments.
Previous retrospective studies have analysed the incidence of atlanto-axial CPP deposition on CT scans done for trauma.
In one study,
the overall prevalence of atlanto-axial deposition reported was 12.5 % and increased reaching 34% in patients above 60 years of age and 49% in patients aged above 80.
Frequency was reported to increase also when calcifications co-exist in the wrist and knee.
Possible,
associated complications reported in the literature include: inflammation,
mass effect causing cord compression and an association with odontoid fractures.
Acute presentation – Crowned Dens Syndrome (CDS)
When CPP deposition in the atlanto-axial joint becomes acutely symptomatic,
it is referred to as “Crowned Dens Syndrome”.
In many but not all cases,
its characteristic triad at presentation includes:
With disease progression,
possible complications include:
Symptoms and signs of Crowned Dens Syndrome can mimic those of:
- polymyalgia rheumatica
- giant cell arteritis
- meningitis
- cervical discitis or spondylodiscitis
- inflammatory spondyloarthritis.
Identification of peri-odontoid calcification on imaging helps to differentiate CDS from these mimics.
Diagnostic Imaging
The diagnostic workup for suspected CDS includes different imaging modalities (table 2).
CT has the highest spatial resolution and sensitivity to detect peri-odontoid calcifications.
MRI has a low sensitivity for calcifications but helps with differential diagnosis and complications.
Plain radiography does not usually show calcifications around the peg and is of limited usefulness.
PET-CT is not part of the routine workup for suspected CDS.
Some advocate its use when initial anti-inflammatory treatment has failed or when there is a suspicion of vasculitis.
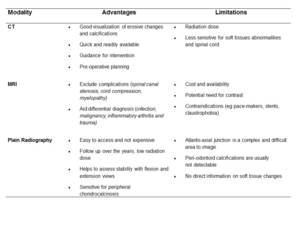
Table 2


: chondrocalcinosis of the menisci (white arrows) and osteoarthritis.
XR Toes - AP view (right): peri-articular/capsular calcification (white arrows).")
 - AP view: chondrocalcinosis at the TFCC (white circle).
XR Hand (right) - AP view: articular calcifications at the MCPJ in the same patient.")
 and axial (right) CT images: focal high attenuation material around the odontoid process.")
