ESSR 2019 / P-0168
Ultrasound screening for developmental dysplasia of the hip: indications, method and illustrative cases
Congress:
ESSR 2019
Poster Number:
P-0168
Type:
Educational Poster
Keywords:
Developmental disease, Education, Ultrasound, Musculoskeletal system, Musculoskeletal joint
Authors:
A. R. Ventosa1, P. M. G. Alves2, A. S. Linhares Moreira2, H. Patricio2; 1Portimão/PT, 2Faro/PT
DOI:
10.26044/essr2019/P-0168

Fig. 1:
Standard coronal plane of the infant hip – anatomical structures.

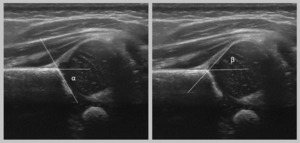
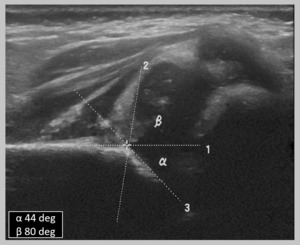
Fig. 2:
Coronal ultrasound image depicting how to measure alpha and beta angles.

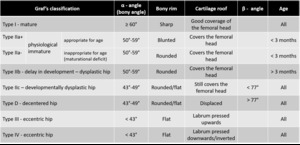
Fig. 3:
Infant hip types according to Graf’s classification.
. References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
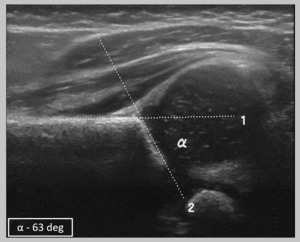
Fig. 4:
Coronal ultrasound image showing how to obtain the measures to calculate the...
. References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
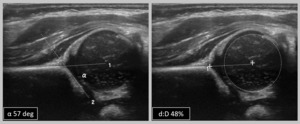
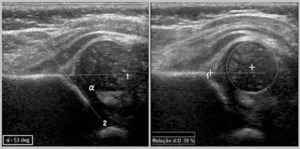
Fig. 5:
Normal/mature hip – Graf type I hip (alpha-angle>60º).

Fig. 6:
Physiological immature hip in a 5-week-old boy – Graf type IIa hip. Both...
. Femoral head coverage is abnormal (<50%). References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
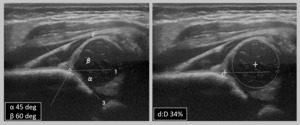
Fig. 7:
Dysplastic hip in a 3-month-old infant – Graf type IIb (alpha-angle 50-59º)....
. Femoral head coverage is also abnormal (<50%). References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
Fig. 8:
Dysplastic hip in a 2-week-old girl – Graf type IIc (alpha-angle 43-49º;...
. References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
Fig. 9:
Decentered hip in a 5-week-old girl – Graf type D hip (alpha-angle 43-49º;...
 References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
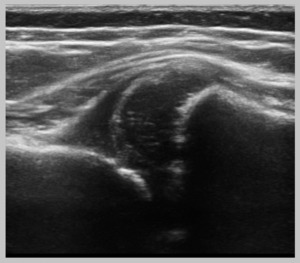
Fig. 10:
Eccentric hip in a 8-week-old girl - Graf type III hip. The bony acetabulum is...
 References: Radiology, Centro Hospitalar Universitário do Algarve - Algarve/PT")
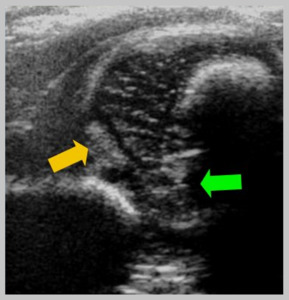
Fig. 11:
Eccentric hip - Graf type IV hip. Labrum - yellow arrow - is inverted and...