ESSR 2019 / P-0178
CT-guided radiofrequency ablation as an effective treatment for osteoid osteoma
Congress:
ESSR 2019
Poster Number:
P-0178
Type:
Educational Poster
Keywords:
Neoplasia, Ablation procedures, CT, Musculoskeletal bone
Authors:
J. S. F. Pinto1, A. M. Alves1, J. Amorim1, J. Mota Louro2, J. Araújo1, C. Fernandes1, M. França1; 1Porto/PT, 2Oporto/PT
DOI:
10.26044/essr2019/P-0178

Fig. 10:
Procedure steps for percutaneous radiofrequency ablation

Fig. 11:
Axial CT image of the proximal tibia depicts an osteoid osteoma with a...

Fig. 12:
Coronal reformatei CT image shows a cortically based sclerotic lesion, a...

Fig. 13:
Axial CT image of the left femural head demonstrates the preferred angle of...

Fig. 14:
Spot CT image obtained after insertion of the cannula. The stylet is removed...

Fig. 15:
Spot CT image show the needle extending beyond the cannula and penetrating the...

Fig. 16:
Spot CT images obtained at successive intervals during needle insertion,...

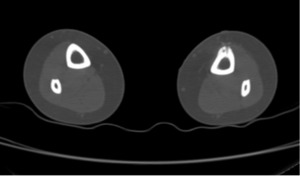
Fig. 17:
Axial CT postprocedural in order to exclude potential complications as soft...