The plain chest radiograph is a valuable test that can support the diagnosis,
confirm the position of tubes and lines,
monitor progression of pulmonary disease,
and detect complications in ARDS.
Although there is considerable overlap,
the radiographic stages of the disease broadly correlate with the histopathological stages.
THE EXUDATIVE PHASE (1-7 days)
CXR
In the first 24-48 h after the initial damage,
CXR may still appear normal.
The exception is if ARDS is triggered by a direct lung injury (for example pneumonia),
in which case consolidation may be observed.
Over the next 24–72 hours rapid deterioration occurs with bilateral,
patchy and symmetrical alveolar opacities progressing to diffuse consolidations,
with a “white lung” appearance in the more severe cases.
Usually,
lung volumes are reduced and air bronchograms are visible.
Cardiogenic edema is the main radiographic differential diagnosis,
but the absence of cardiomegaly,
septal lines,
or pleural fluid and the presence of peripheral alveolar opacities all favor ARDS.
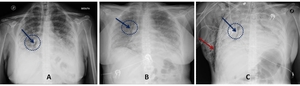
Fig. 5: A 52-year-old female with hypoxaemia and shortness of breath: ARDS exudative phase. CXR at admission (A) demonstrates bilateral, symmetrical and peripheral alveolar opacities. Air bronchogram is visible at right lung base (blu arrow). Five-days follow-up CXR (B) demonstrating bilateral homogeneous air space opacification and a small flap of pneumomediastinum (blu arrow). Six-days follow-up CXR (C) demonstrates bilateral and diffuse consolidations with a “white lung” appearance. The flap of pneumomediastinum appears increased (blu arrow) and a largest flap of subcutaneous emphysema occurs in the right lateral chest wall, expression of complication (red arrow). Endotracheal tube and right pleural drainage tube are present.
References: Radiology, University Hospital of Chieti - Chieti/IT
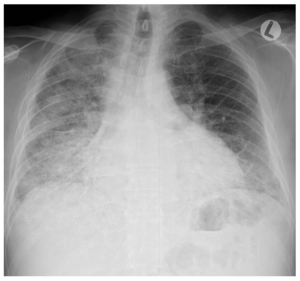
Fig. 6: CXR in a 51-year-old male hospitalized for severe hypoxaemia, fever and cough shows diffuse air space opacification in the right lung, supported by pneumonia (direct lung injury). In pulmonary ARDS the opacities tend to be asymmetrical, with non-dependent consolidations. It must be kept in mind that the presence of consolidations in non-dependent areas or the appearance of a new area of consolidation may be a sign of both a pre-existing pneumonia and a new ventilation-associated pneumonia.
References: Radiology, University Hospital of Chieti - Chieti/IT
THE EXUDATIVE PHASE (1-7 days)
CT
The classical CT appearance of acute phase ARDS is that of opacification that demonstrates an antero-posterior density gradient within the lung,
with dense consolidation in the most dependent regions,
merging into a background of widespread ground-glass attenuation and then normal or hyperexpanded lung in the non-dependent regions.
Ground-glass opacification on CT is a non-specific sign that reflects an overall reduction in the air content of the affected lung.
In the case of acute ARDS,
this is likely to represent edema and protein within the interstitium and alveoli.
Another important observed feature in acute ARDS is bronchial dilatation within areas of ground-glass opacification.
While this may be an indicator of the development of early fibrosis (so-called traction bronchiectasis),
the sign cannot be taken as conclusive proof of fibrosis because the reversal of bronchial dilatation in the later stages of ARDS is a well recognized phenomenon.
CT proved that the acute exudative lesions in ARDS are not randomly distributed (as was thought on the basis of chest radiographs) but have a gravitationally dependent gradient,
with more consolidation in the posterobasal regions,
as a result of compressive gravitational forces.
The theory is supported by the fact that when the position of a patient with ARDS is changed from supine to prone,
the density gradient quickly redistributes accordingly.
In the nondependent portions,
lung may be of normal attenuation,
or it may be even lower if the patient is being mechanically ventilated.
The identification of dense consolidation in nondependent areas of the lung should always alert the clinician to the possibility of infective consolidation,
either from a pre-existing pneumonia (which may have been the precipitating condition in ARDS) or new ventilation-associated pneumonia.
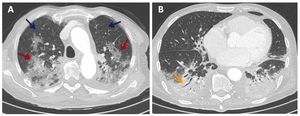
Fig. 7: Fifty-year-old male with hypoxaemia and shortness of breath; ARDS exudative phase. CT scan (A) at the level of the aortic arch shows in the upper lobes areas of normal attenuation (blu arrows) and areas of ground-glass opacification (red arrows). CT image (B) shows in the lower lobes bilateral consolidations with air bronchogram (orange arrow) in the dependent portions, as a result of compressive gravitational forces.
References: Radiology, University Hospital of Chieti - Chieti/IT
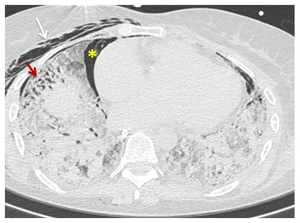
Fig. 8: CT scan shows bilateral reticulation and ground-glass opacification, containing areas of bronchial dilatation in the lower lobes (red arrow). In the acute phase of ARDS, bronchial dilatation may indicate fibrosis or may be reversible. Note also the pneumomediastinum (yellow asterisk*) and right subcutaneous emphysema (white arrow).
References: Radiology, University Hospital of Chieti - Chieti/IT
PROLIFERATIVE OR INTERMEDIATE PHASE (8–15 DAYS)
CXR
After the rapid development of radiographic changes in the acute phase of ARDS,
the appearances usually stabilize and remain static for a variable length of time.
During the intermediate phase,
diffuse coarse reticular opacities may develop on the chest radiograph,
although this does not imply irreversible fibrosis,
as the opacities may resolve.
It is important to be aware of this stable period in the radiographic appearances of the disease,
as new air space opacities are likely to represent superadded infection or other complications outside the natural history of ARDS.
Reticular opacities may appear in the diffuse and persisting background of alveolar opacities.
CT
In this phase,
the extent of CT opacities (80% of lung volume),
along with the presence of bronchiectasis,
honeycombing and signs of pulmonary hypertension (dilatation of pulmonary arteries and right ventricle) indicates early fibrosis and predicts mortality.
Recurrent exudative episodes can occur,
resulting in mixed radiological appearances.
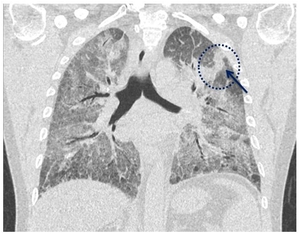
Fig. 9: Fifty-one year-old man, hospitalized for severe hypoxaemia; ARDS proliferative phase. MPR coronal reconstruction shows bilateral ground-glass opacification with an area of consolidation in the left upper lobe (blu arrow).
References: Radiology, University Hospital of Chieti - Chieti/IT
FIBROTIC OR LATE PHASE (> 15 DAYS)
CXR
Although the death rate is declining (while still 50%),
the long-term disability in survivors is considerable.
If the patient survives the acute phase of ARDS,
most radiographic abnormalities begin to resolve in the late phase.
The speed and duration of recovery are variable and depend on various factors,
including comorbidities.
In surviving patients,
pulmonary opacities tend to wane with unpredictable speed.
The final result could be a normal looking lung or a pattern characterized by lung volume reduction and coarse reticulations.
FIBROTIC OR LATE PHASE (> 15 DAYS)
TC
After the acute phase,
CT appearances are variable.
Although complete resolution of abnormalities may occur,
the more typical later stage CT appearances are that of a coarse reticular pattern and ground-glass opacification in the anterior (nondependent) part of the lungs.
In this setting it is likely that the ground-glass opacities represent areas of fine fibrosis,
which are too small to be resolved on CT.
Fibrosis develops in these patients as a sequelae of barotrauma secondary to mechanical ventilation in the nondependent lung,
with consolidation and atelectasis conferring relative protection on the more dependent regions.
The majority of patients had a diffuse distribution of disease,
with only approximately a third having the more classical exclusively anterior changes.
A smaller number (18%) were also reported to have exclusively posterior abnormalities.
The study also reiterated the finding that airways disease (traction bronchiectasis) was common,
again implying underlying lung fibrosis in these patients.
Pulmonary cysts of varying sizes and bullae are also features of the later stages of ARDS and probably develop as a result of prolonged ventilation.
However pulmonary cysts are also know to arise secondary to pneumonia and do not necessarily have to be associated with an episode of prolonged ventilation.
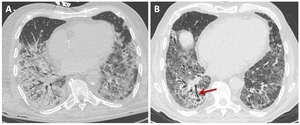
Fig. 10: 79 years old male with hypoxaemia and shortness of breath. CT scan ( A) at the level of the left pulmonary vein shows bilateral ground-glass opacities and consolidation in the lower lobes. Two months follow-up chest CT (B) demonstrates reduction of ground-glass opacities in the posterobasal regions of lungs with intralobular interstitium thickening. Note some traction bronchiectasis (red arrow) and nearly a pulmonary cyst in the right lower lobe in relation to fibrotic evolution.
References: Radiology, University Hospital of Chieti - Chieti/IT
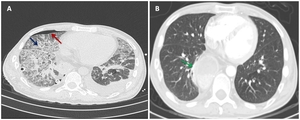
Fig. 11: A 50-year-old male underwent to resection of distal esophagus for cancer. CT scan shows volume reduction of the lungs, bilateral ground-glass opacification with thickening of interlobular septa (crazy paving, blu arrow) and consolidation. Note also the right pneumothorax (red arrow), the left pleural effusion and the right thoracic drainage tubes. Five-months follow-up chest CT (B) shows no significant parenchymal abnormalities. Note also distal esophagus surgical findings (green arrow).
References: Radiology, University Hospital of Chieti - Chieti/IT
INDICATIONS FOR CHEST RADIOGRAPHY AND CT IN ARDS
CXR
- Detection of clinically occult complications (e.g.
nosocomial pneumonia)
- Confirmation of a clinically suspected complication (iatrogenic or otherwise)
- Monitoring progression or regression of radiographic opacities
CT
- As a problem-solving tool in patients with complex appearances on plain radiography
- For quantification of the extent of lung abnormality in patients with equivocal plain radiographic changes
- As an aid to determining the aetiology of ARDS (i.e.
pulmonary versus extrapulmonary)
- Identification of significant areas of dependent dense parenchymal opacification (compression atelectasis) in patients being considered for prone ventilation
- In clinical trials of new drug therapies of ARDS
- Determination of the extent of lung abnormality in ARDS survivors
- CT is the gold standard to target PEEP by assessing recruitment and hyperinflation
CT AS A MEANS TO DIRECT VENTILATION
The mainstay of management in ARDS is mechanical ventilation.
This life-saving therapy is also an invasive one,
with potential to cause barotrauma and long-term damage to the lungs.
Recruitment is a term that refers to the number of previously collapsed acini that can be inflated for a given pressure.
Increasing PEEP recruits more lung at the higher pressure end of the spectrum.
However,
increased ventilation pressure can cause barotrauma to the lung that would have successfully been ventilated at lower pressures.
This means that there is a trade-off between recruiting more acini for gas exchange and causing ventilator- related lung injury.
On CT,
collapsed lung can be readily identified and in the case of ARDS this is likely to be dependent lung,
collapsed under the increased weight of the overlying lung.
By acquiring CT images at different ventilator settings,
the assessment of the potential for recruitment can be made by identifying the extent of atelectatic lung and its response to ventilation.
CT clearly shows the morphological basis of the PEEP response,
because it will be positive when there is prevalence of edema-related atelectasis and negative when there is prevalence of consolidation.
Furthermore the prone positioning is important to improve ventilation to the dorsal areas of the lungs by reducing the vertical pressure gradient.
The improvement of the ventilation/perfusion ratio is determined by positioning the ventilated alveoli in the dependent regions,
where perfusion gravitationally predominates,
and by decreasing the overdistension of ventral areas,
with a reduction of alveolar wall injury.
COMPLICATIONS
Superimposed cardiac failure,
pneumonia,
pulmonary embolism and hypertension,
ventilator-induced lung injury,
malposition of tubes may worsen the clinical evolution.
Early signs of barotrauma often correspond to interstitial emphysema and subpleural cystic air spaces.
Subsequently,
imaging studies can demonstrate the development of pneumomediastinum,
pneumothorax (often hypertensive in mechanically ventilated patients) and subcutaneous emphysema. In an ARDS patient who is deteriorating,
CT can detect various ventilation-associated complications and foci of infection that may not be apparent on the antero-posterior,
supine,
intensive care unit chest radiograph.
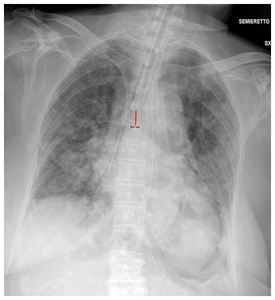
Fig. 12: CXR in a 64-year-old male with ARDS shows malpositioned endotracheal tube that is 1.8 cm above the carina.
References: Radiology, University Hospital of Chieti - Chieti/IT
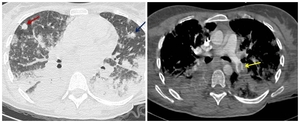
Fig. 13: A 38-year-old female after a caesarean section presented to the Critical Care Unit with hypoxaemia, shortness of breath and septic fever. CT scan (A) demonstrates bilateral ground-glass opacification in the upper lobes and consolidations in the lower lobes. Note some consolidative nodular lesions (red and blu arrows) suspect for septic emboli. CT scan (B) after contrast medium infusion of the same patient shows defect of filling in the left lower lobar artery to refer to thrombus (yellow arrow).
References: Radiology, University Hospital of Chieti - Chieti/IT

 demonstrates bilateral, symmetrical and peripheral alveolar opacities. Air bronchogram is visible at right lung base (blu arrow). Five-days follow-up CXR (B) demonstrating bilateral homogeneous air space opacification and a small flap of pneumomediastinum (blu arrow). Six-days follow-up CXR (C) demonstrates bilateral and diffuse consolidations with a “white lung” appearance. The flap of pneumomediastinum appears increased (blu arrow) and a largest flap of subcutaneous emphysema occurs in the right lateral chest wall, expression of complication (red arrow). Endotracheal tube and right pleural drainage tube are present. References: Radiology, University Hospital of Chieti - Chieti/IT")
. In pulmonary ARDS the opacities tend to be asymmetrical, with non-dependent consolidations. It must be kept in mind that the presence of consolidations in non-dependent areas or the appearance of a new area of consolidation may be a sign of both a pre-existing pneumonia and a new ventilation-associated pneumonia. References: Radiology, University Hospital of Chieti - Chieti/IT")
 at the level of the aortic arch shows in the upper lobes areas of normal attenuation (blu arrows) and areas of ground-glass opacification (red arrows). CT image (B) shows in the lower lobes bilateral consolidations with air bronchogram (orange arrow) in the dependent portions, as a result of compressive gravitational forces. References: Radiology, University Hospital of Chieti - Chieti/IT")
. In the acute phase of ARDS, bronchial dilatation may indicate fibrosis or may be reversible. Note also the pneumomediastinum (yellow asterisk*) and right subcutaneous emphysema (white arrow). References: Radiology, University Hospital of Chieti - Chieti/IT")
. References: Radiology, University Hospital of Chieti - Chieti/IT")
 at the level of the left pulmonary vein shows bilateral ground-glass opacities and consolidation in the lower lobes. Two months follow-up chest CT (B) demonstrates reduction of ground-glass opacities in the posterobasal regions of lungs with intralobular interstitium thickening. Note some traction bronchiectasis (red arrow) and nearly a pulmonary cyst in the right lower lobe in relation to fibrotic evolution. References: Radiology, University Hospital of Chieti - Chieti/IT")
 and consolidation. Note also the right pneumothorax (red arrow), the left pleural effusion and the right thoracic drainage tubes. Five-months follow-up chest CT (B) shows no significant parenchymal abnormalities. Note also distal esophagus surgical findings (green arrow). References: Radiology, University Hospital of Chieti - Chieti/IT")

 demonstrates bilateral ground-glass opacification in the upper lobes and consolidations in the lower lobes. Note some consolidative nodular lesions (red and blu arrows) suspect for septic emboli. CT scan (B) after contrast medium infusion of the same patient shows defect of filling in the left lower lobar artery to refer to thrombus (yellow arrow). References: Radiology, University Hospital of Chieti - Chieti/IT")