RANZCR ASM 2010 / R-0062
Heterotopic Pregnancy – Case reports and a short review of literature
This poster was originally presented at the RANZCR Annual Scientific Meeting 2010, October 14-17, in Perth/AU.
Congress:
RANZCR ASM 2010
Poster Number:
R-0062
Type:
Educational Exhibit
Keywords:
Obstetrics, Foetus, Diagnostic procedure, Ultrasound-Colour Doppler, Ultrasound, Pelvis, Obstetrics (Pregnancy / birth / postnatal period), Genital / Reproductive system female
Authors:
T. Mathews, J. Hanson, R. Rattan, T. Durrance, S. Hiscock; NSW/AU
DOI:
10.1594/ranzcr2010/R-0062

Fig. 1:
Coexistent intra and extrauterine gestations

Fig. 2:
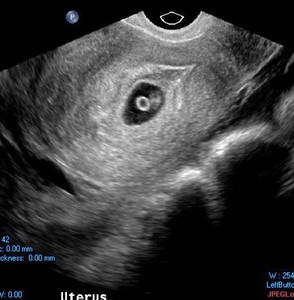
Transvaginal ultrasound image of a viable intrauterine foetus

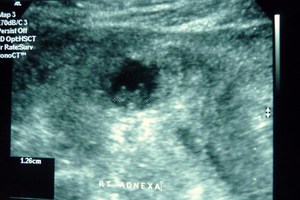
Fig. 3:
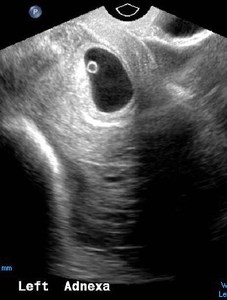
Transvaginal ultrasound image of a left adnexal mass showing a yolk sac within...

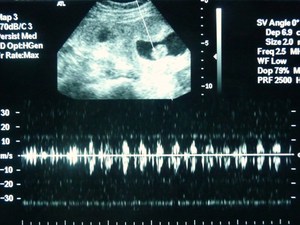
Fig. 4:
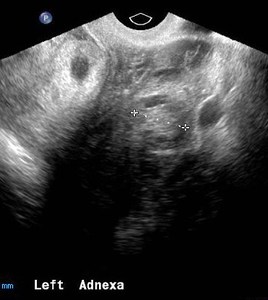
Ultrasound image of a complex left adnexal mass showing peripheral blood flow

Fig. 5:
Transabdominal image showing an intrauterine gestation and a coexistent left...

Fig. 6:
Transabdominal ultrasound image demonstrating a viable intrauterine gestation

Fig. 7:
Transabdominal ultrasound image demonstrating a viable intrauterine gestation

Fig. 8:
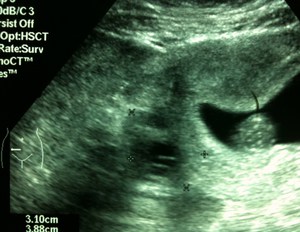
Transabdominal ultrasound image showing fluid in Morrison's pouch

Fig. 9:
Ultrasound of a complex right adnexal lesion. Magnified view suggests a foetal...