Congress:
RANZCR ASM 2013
Type:
Educational Exhibit
Keywords:
Neoplasia, Cancer, Surgery, MR, CT, Head and neck, Ear / Nose / Throat, Pathology
Authors:
L. L. Wang1, D. T. Wang2, I. Bhutani1, R. Cornelius1; 1Cincinnati/US, 2Melbourne/AU
DOI:
10.1594/ranzcr2013/R-0126
Background
Salivary gland neoplasms
- Incidence 0.4-2.5 in 100,000 [1]
- Majority (80%) are parotid gland tumours
- Account for approximately 3% of head and neck tumours [2]
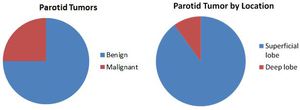
Fig. 1: Parotid Tumor
Benign versus malignant
By location
References: University Hospital Cincinnati
Parotid gland tumours [3]
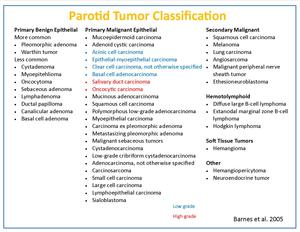
Fig. 2: Parotid tumor classification
References: University Hospital Cincinnati
Routes of spread
- Incidence of distant metastases from parotid primary malignant tumor varies from 20-40% [4]
- Sites include lung,
long bones,
brain and liver
- Pleomorphic adenoma rarely spreads,
but there are 42 reports in literature of metastasising pleomorphic adenoma [5]
- SCC and malenoma from the cheek and temple region can metastasise to intraparotid lymph nodes [6,
7]
Clinical examination
- Deep lobe cannot be palpated
- Pain & facial nerve involvement are more suggestive of malignant tumor
- Also rapid enlargement in pleomorphic usually suggests carcinoma ex
- However,
overall,
clinical signs are not reliable
- Some paper even report that clinical signs and symptoms were of no value in distinguishing between malignant and benign parotid tumors [8]
- Conservative parotidectomy is the most widely accepted surgical treatment for benign tumors
Imaging of the Parotid Gland
- 5 lobules
- – 3 superficial
- – 2 deep
- Accessory parotid glandular tissue seen in 20% of population,
usually anterior to the main parotid gland
- The only major salivary gland that contains intraglandular lymphoid tissue
- May demonstrate lymph nodes
- May receive drainage from the palatine tonsil
- – ->level IIa and IIb lymph nodes
- Multicentricity may influence recurrence rate
- – Role of imaging to look for other lesions
- – Metastases
- A poorly defined tumour boundary with evidence of local invasion was the best indicator of malignancy in a series of 42 patients with primary malignant parotid disease [9]
- No imaging feature that could reliably predict the histology [9]
– More frequently used in Australia and Europe compared to the USA
– Can be done in ENT office
– FNA can be performed
– Readily available
– Good evaluation of local spread and deep lobe
– Evaluation of facial nerve,
deep lobe extension
– Parapharyngeal space visualization
– More reliable in identifying local infiltration [9]
– Does not reliably differentiate benign from malignant tumors
– Useful in picking up incidental lesions
– Use for the assessment of metastatic disease or look for primary disease metastasized to parotid
– Little role in tumor assessment
