PRIMARY BENIGN EPITHELIAL
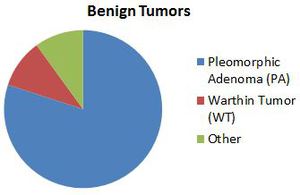
Fig. 3: Benign parotid tumors
References: University of Cincinnati Hospital Medical Center
- Pleomorphic adenoma is the commonest parotid tumor by far
- These ‘benign’ tumors of the parotid can harbor or become malignant,
(with the exception of WT) and are surgically removed
- Imaging features of pleomorphic adenoma and Warthin tumor are better documented in the literature
- The other tumors have variable imaging features
Pleomorphic Adenoma (PA)
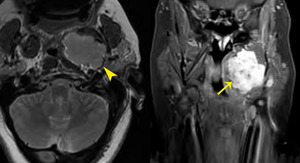
Fig. 4: Pleomorphic adenoma
53 year old female
T2 WI (left) T1 post contrast FS MRI (right) shows a fairly homogeneous enhancing mass (arrow) with hyperintense T2 signal and a well-defined low T2 signal capsule (arrowhead).
References: University of Cincinnati Hospital Medical Center
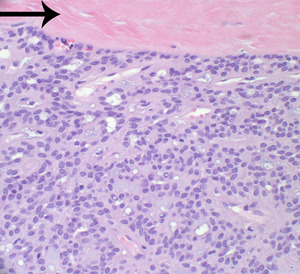
Fig. 5: An encapsulated (note the fibrous tissue [arrow]) monomorphic population of epithelial cells forms small tubules in a myoid and chondroid stroma.
References: University of Cincinnati Hospital Medical Center
- Also known as benign mixed tumor
- Most common benign tumor in adults 45-80%
- Middle aged females
- Palpable slow growing mass
- Superficial 90% > deep lobe 10%
- Can grow to 6-8 cm when in deep lobe.
- Dystrophic calcification may be present in large pleomorphic adenomas.
- Variable rate of recurrence 1-50%
- Malignant degeneration 2-25%
- Associated malignancies: carcinoma ex-PA*,
malignant mixed tumor and metastasizing mixed tumor
- Must be excised completely
- CT typically shows
- Delayed enhancement [10]
*malignant change of a PA or a malignant tumor in a patient who previously underwent surgery for a PA
[11]
Warthin Tumor
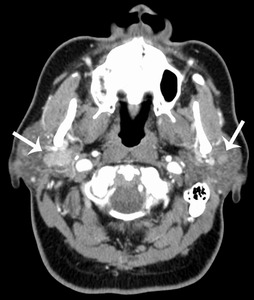
Fig. 6: 58 year old female
Warthin tumor
CT with contrast shows well-defined enhancing bilateral parotid masses (arrows). The right parotid mass has deep lobe extension.
References: University of Cincinnati Hospital Medical Center
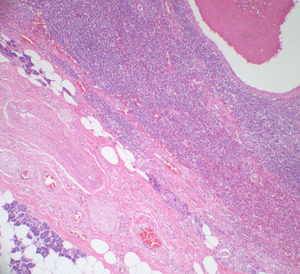
Fig. 7: There is a cystic space lined by a bilayer of oncocytic cells surrounded by abundant lymphoid tissue. Note the adjacent parotid parenchyma.
References: University of Cincinnati Hospital Medical Center
- A.k.a.
cystadenoma lymphomatosum
- Commonly in older male smokers
- Increasing in incidence,
thought to be related to increased rate of smoking in women
- Commonly within parotid tail,
superficial to angle of mandible.
- Malignant degeneration <1%
- No calcification
- Cystic component in 30%
- Pain 10%
- Mural nodule
- Multiple,
unilateral or bilateral synchronous or metachronous in 20%,
important to recognize pre-operatively
- Can have increased FDG-PET uptake and 99mTc studies [11,
12]
- Management is controversial [13,
14]
Papillary Oncocytic Cystadenoma
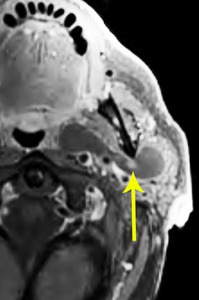
Fig. 8: Papillary oncocytic cystadenoma
82 year old male
Post-contrast T1 FS shows a fluid signal non-enhancing lesion with a small enhancing nodule (arrow), involving both superficial and deep lobe of the left parotid, extending behind the angle of the mandible and across the anterior margin of the internal carotid artery.
References: University of Cincinnati Hospital Medical Center
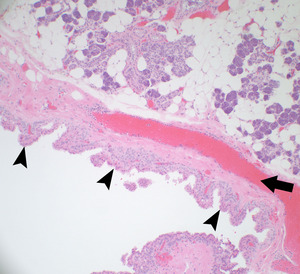
Fig. 9: There is a cystic space lined by papillary structures (arrowheads) (note the fibrovascular cores [arrow]) containing oncocytic epithelium. Note the adjacent parotid parenchyma.
References: University of Cincinnati Hospital Medical Center
- Minor > major salivary gland
- Rarely seen in parotid gland
- Women > men
- >50 years of age
- Painless insidious mass
- Resembles Warthin tumor on histology
PRIMARY MALIGNANT EPITHELIAL
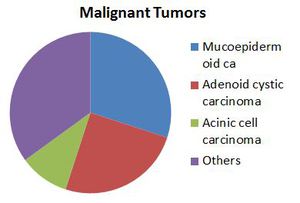
Fig. 10: Malignant Tumors of Parotid
References: University of Cincinnati Hospital Medical Center
- Malignant epithelial tumors of the parotid differ in incidence compared to minor salivary gland tumors
- There is large number of subtypes,
accounting for the large proportion of ‘others’
- Mucoepidermoid and adenoid cystic are the most common types
- Due to a large number of ‘others’,
case series are difficult to obtain
- Imaging features are also not reliable
- The assessment of a suspected malignant parotid tumor by pre-operative imaging is mainly to determine
- Margins
- Structures involved
- Nodal and/or perineural metastases
- The incidence of occult metastases in clinically N0-elective neck dissection was 22% [15].
- A routine elective neck dissection in all N0 parotid carcinomas is suggested by this study with 98 subjects [15]
Mucoepidermoid Carcinoma
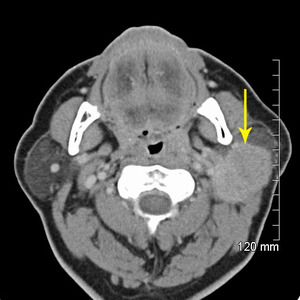
Fig. 11: Mucoepidermoid carcinoma
Post contrast CT shows mostly well-defined homogeneously enhancing mass occupying most of the left superficial parotid. The posterior margin is slightly less well-defined.
References: University of Cincinnati Hospital Medical Center
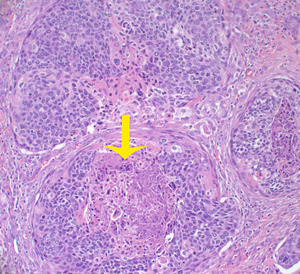
Fig. 12: Nests of epidermoid-type cells with intracellular mucin. Note the foci of necrosis (arrow).
References: University of Cincinnati Hospital Medical Center
- Superficial >> deep
- Radiation risk factor
- Most common parotid malignancy
- 10% of all salivary gland tumors,
30% of all salivary gland malignancies
- Frequently young adults
- Low grade: well circumscribed
- High grade: poor margins,
invasion
- May have calcification
- Metastasize to lymph nodes,
bone and lung
- 40% symptomatic
- Perineural tumor spread along facial nerve
[11]
Adenoid Cystic Carcinoma
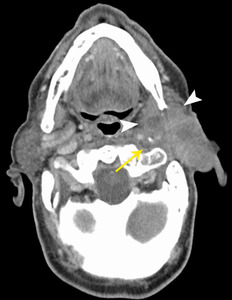
Fig. 13: Adenoid cystic carcinoma
81 year old male. Post contrast CT shows an irregular, partially solid, partially cystic mass (arrowheads) involving both the superficial and deep lobes of the right parotid. The carotid artery is displaced posteromedially (arrow) and has an ill-defined margin with the mass.
References: University of Cincinnati Hospital Medical Center
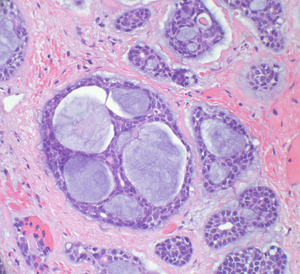
Fig. 14: Epithelial cells with scant cytoplasm form cribriform (cookie-cutter) formations in ducts that contain a basophilic basement membrane-like material.
References: University of Cincinnati Hospital Medical Center
- 2-6% of parotid tumors
- Slow-growing
- Long standing pain
- Variable appearance
- May demonstrate skull base invasion via perineural extension
- The most common distant metastasis site from primary parotid carcinoma was the lung [16,
17]
Adenocarcinoma,
Mucinous
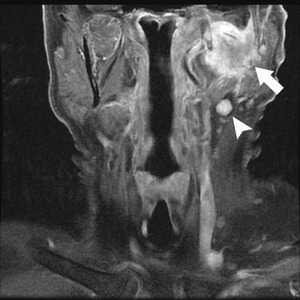
Fig. 15: Adenocarcinoma, mucinous
Post contrast T1 WI FS image shows a large ill-defined enhancing mass (arrow) centered in the left parotid, with abnormal ipsilateral nodes (arrowhead).
References: University of Cincinnati Hospital Medical Center
- Very little literature about mucinous adenocarcinoma of the parotid
- Adenocarcinoma
- -Typical 71%
- -Papillary 12%
- -Mucinous 12%
Salivary Duct Carcinoma (SDC)
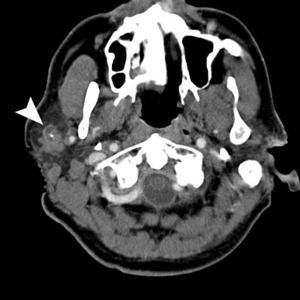
Fig. 16: Salivary duct carcinoma
Post contrast CT shows an irregular, ill defined, mildly enhancing mass in the right parotid status post biopsy. There is a focus of dystrophic calcification centrally.
References: University of Cincinnati Hospital Medical Center
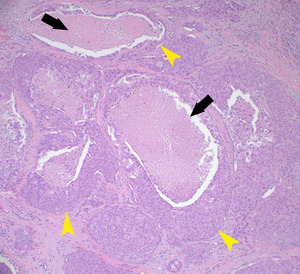
Fig. 17: Islands of variably pleomorphic epithelial cells form ducts (arrowheads) and contain intraluminal “comedo” necrosis (arrows) [intraductal component]; the ducts are set in a desmoplastic stroma [invasive component]. SDC are histologically similar to ductal carcinoma of the breast. Flat sheets of tumor cells with cribiform pattern is a characteristic feature.
References: University of Cincinnati Hospital Medical Center
- High grade
- Aggressive growth with early regional and distant metastasis (lung,
bone,
liver)
- Older male
- Facial paralysis 40-60%
- Parotid most common site
- 70% die within 3 years of diagnosis [18]
- Sarcomatoid SDC characterized by carcinomatous and sarcomatoid elements
- 25% patients die within 2 years of completion of treatment [19]
- Poor survival despite radical parotidectomy,
neck dissection and adjuvant radiotherapy
Primary Squamous Cell Carcinoma (SCC)
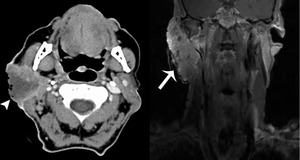
Fig. 18: Primary SCC
60 year old male. CT with contrast and post contrast T1 WI FS. A large predominately hypoattenuating mass (arrow) in the right parotid gland that demonstrates irregular peripheral enhancement. The lesion is inseparable from the posterior aspect of the masseter muscle. The mass extends to the superficial skin with an irregular surface and deep into the retromandibular region. The overlying skin is ulcerated (arrowhead). There are necrotic ipsilateral neck lymph nodes (not shown).
References: University of Cincinnati Hospital Medical Center
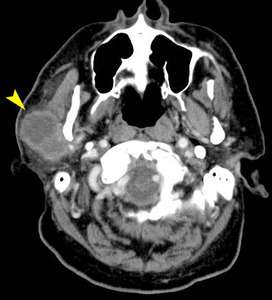
Fig. 20: A sheet of epithelioid cells with ample eosinophilic cytoplasm with scattered dyskeratotic cells (arrowhead) in the background. Note the intercellular bridges (small arrow & insert).
References: University of Cincinnati Hospital Medical Center
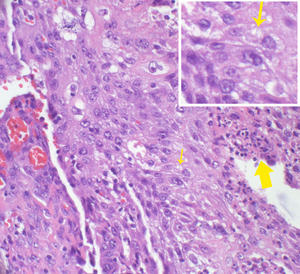
Fig. 19: A sheet of epithelioid cells with ample eosinophilic cytoplasm with scattered dyskeratotic cells (arrowhead) in the background. Note the intercellular bridges (small arrow & insert).
References: University of Cincinnati Hospital Medical Center
- Primary parotid SCC is very rare
- Most of SCC found in parotid are metastases
Acinic Cell Carcinoma
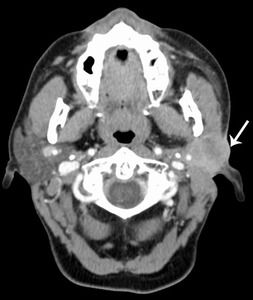
Fig. 21: Acinic cell carcinoma
56 year old female. CT with contrast shows a fairly homogeneously enhancing mass in the left parotid, involving the skin (arrow) and deep extension to the carotid sheath.
References: University of Cincinnati Hospital Medical Center
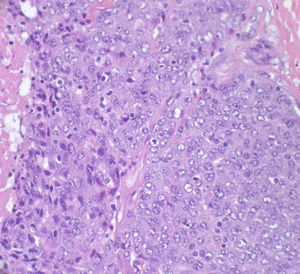
Fig. 22: A sheet of syncytial polygonal cells with prominent nucleoli and granular amphophilic cytoplasm
References: University of Cincinnati Hospital Medical Center
- ACC is the 3rd most common epithelial salivary gland malignancy
- Low grade with predilection for females
- Presents at a relatively younger age
- Tendency to recur and metastasize
- Most common salivary malignancy to be bilateral
- Mortality 1%-26%
[20]
Metastasizing Pleomorphic Adenoma
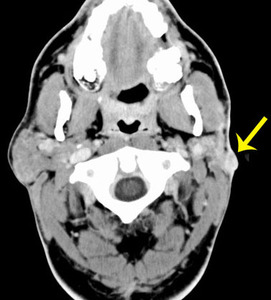
Fig. 23: Metastasizing pleomorphic adenoma
51 year old male with a history of superficial parotidectomy a year prior to this presentation. Post contrast CT shows small solid enhancing nodule in the superficial lobe of the left parotid. Pathology demonstrates local metastasis to neck lymph nodes. Distant metastases were also present in the lung.
References: University of Cincinnati Hospital Medical Center

Fig. 25: Pleomorphic adenoma with carcinoma ex
CT with contrast . 48 year old female with a partially calcified mass in the superficial lobe of the right parotid gland. The patient had a PA excised previously. The pathology showed carcinoma.
References: University of Cincinnati Hospital Medical Center
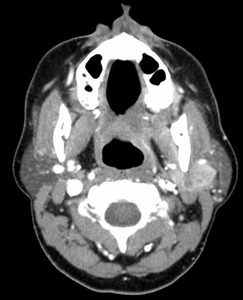
Fig. 24: Pleomorphic adenoma with carcinoma ex
CT with contrast . 48 year old female with a partially calcified mass in the superficial lobe of the right parotid gland. The patient had a PA excised previously. The pathology showed carcinoma.
CT with contrast. The patient has a history of prior pleomorphic adenoma resection years ago. The pathology of the recurrent tumor was consistent with carcinoma when excised.
References: University of Cincinnati Hospital Medical Center
- Pleomorphic adenoma can metastasize,
even though it is benign.
- WHO defines MPA as histologically benign PA that inexplicably manifests local or distant metastasis.
- On average,
occurs 16 years after the treatment of the initial benign PA [5]
- Associated mortality up to 22% [5]
- An investigation of a recurrent PA should include a search for distant metastases.
- Treatment is resection of the metastasis,
where possible.
- 81% with MPA have a history of at least 1 local recurrence of PA prior to the detection of distant metastasis [5]
Adenocarcinoma
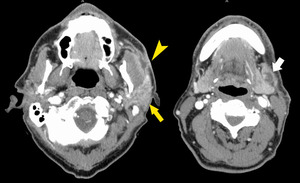
Fig. 26: Adenocarcinoma
59 year old male. CT with contrast. Large low density mass involving the superficial lobe of the right parotid, extending to the left masseter muscle and the parotid duct. Pathology shows perineural invasion by adenocarcinoma.
References: University of Cincinnati Hospital Medical Center
- Parotid adenocarcinoma is very rare.
- It has been reported to arise from Warthin tumors [21,
22]
Oncocytic Carcinoma
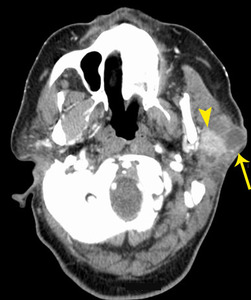
Fig. 27: Oncocytic carcinoma
65 year old female. CT with contrast shows lobulated tumor with necrotic areas(arrow) and an enhancing solid nodule (arrowhead) in the superficial lobe of the left parotid gland.
References: University of Cincinnati Hospital Medical Center
- 5 year survival 69%
- Elective neck dissection is recommended for patients with cancer stage T2 to 4
- Surgery with postoperative I-125 brachytherapy leads to good local control [23]
HEMATOLYMPHOID
Lymphoma
- Mucosa-associated lymphoid tissue lymphoma
- Multiple well-circumscribed homogenous masses with lymphadenopathy
- Necrosis in high grade
- Sjogren syndrome – 40 x higher
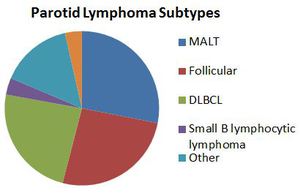
Fig. 28: Primary Parotid Lymphoma
References: University of Cincinnati Hospital Medical Center
- 2% of all salivary gland tumors are lymphomas
- All non-Hodgkin lymphoma
- Mostly with no B symptoms
- Stage I or II mostly (70%)
[3]
Extranodal Marginal Zone Lymphoma
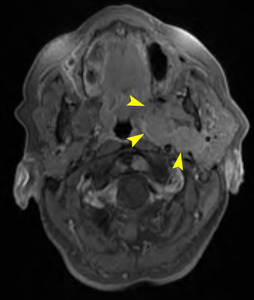
Fig. 29: Extranodal marginal zone lymphoma
74 year old female. Post contrast T1 WI FS shows
solid enhancing deep lobe mass (arrowheads) with effacement of the parapharyngeal space. The carotid sheath is displaced posteriorly.
References: University of Cincinnati Hospital Medical Center
- Primary parotid lymphoma is rare
- Parotid lymphomas are mostly extranodal marginal zone B-cell.
- Usually elderly men
- Biopsy regional nodes (if abnormal) preferred
- Primary lymphoma is bilateral in 2.3%
- Facial nerve preservation is possible if frozen section shows lymphoma [24]
Follicular Lymphoma
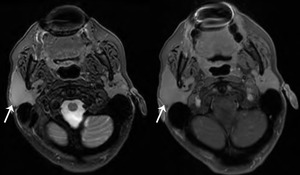
Fig. 30: Follicular lymphoma
59 year old female. Post contrast T1 FS.
Homogeneously enhancing 3.5 x 2 x 2 cm mass involving the superficial and deep lobes. It has a normal soft tissue planes between the right masseter muscle and pterygoid muscles.
References: University of Cincinnati Hospital Medical Center
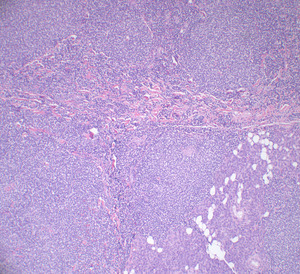
Fig. 31: A sheet-like pattern of neoplastic lymphoid cells recapitulating mature follicles is diffusely involving the parotid parenchyma
References: University of Cincinnati Hospital Medical Center
SECONDARY MALIGNANT
Metastatic Disease to the Parotid
- Important to distinguish between primary versus metastasis malignant tumors for therapy and prognosis
- There are intra and peri-parotid lymph nodes
- In the setting of head & neck malignancy
- Look for perineural spread along CN7
- Parotid nodes are 1st order nodes for skin of upper face,
external ear,
scalp
- Hematogenous metastases rare
- Pathological distinction is difficult in
- – Clear cell carcinoma
- – Small cell carcinoma
- – Undifferentiated carcinoma
- – Squamous cell carcinoma
- – Ductal mammary carcinoma
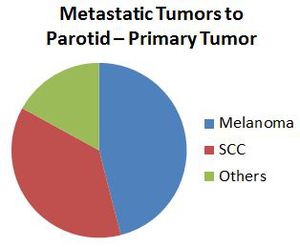
Fig. 32: Metastatic Tumors to Parotid – Primary Tumor
References: University of Cincinnati Hospital Medical Center
- Parotid gland has a rich lymphatic network which drains the temple area and the cheek region
- Parotid nodes then drain into upper cervical nodes
- 15-20 periparotid nodes
- 4-5 deep lobe nodes
Squamous Cell Carcinoma Metastasis
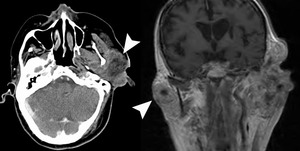
Fig. 33: SCC metastasis
70 year old male. CT post contrast and T1 FS.
Large relatively centrally hypodense, mildly peripheral enhancing masses (arrow) in both parotid glands in a patient with a history of scalp SCC.
References: University of Cincinnati Hospital Medical Center
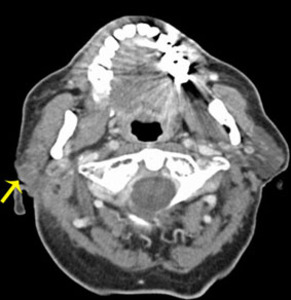
Fig. 34: SCC metastasis
80 year old man with a history of stage IV renal cell carcinoma, nephrectomy, skin squamous cell carcinoma presented with right parotid swelling. CT with contrast shows a mildly enhancing soft tissue mass (arrow) in the superficial lobe of the right parotid gland, extending to the skin.
References: University of Cincinnati Hospital Medical Center
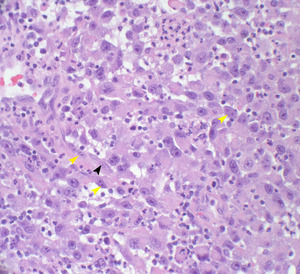
Fig. 35: Sheet of variably pleomorphic epithelial cells with prominent nucleoli. Some cells have spindle cell morphology (black arrowhead) and some are multinucleated (yellow arrowheads). There are atypical pathological features, with keratinization in some areas.
References: University of Cincinnati Hospital Medical Center

Fig. 36: SCC metastasis
84 year old female. CT with contrast shows a well-defined, peripherally enhancing, centrally non-enhancing necrotic mass in the superficial right parotid gland, consistent central necrosis.
References: University of Cincinnati Hospital Medical Center
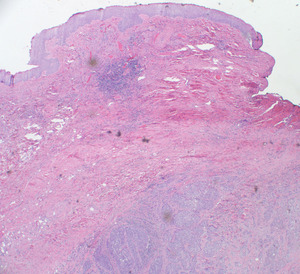
Fig. 37: Nests of malignant epithelial cells are in the subcutaneous tissue. Note no origin of tumor from the epidermis.
References: University of Cincinnati Hospital Medical Center
- Metastases are far more common than 1° SCC
- 5% of cutaneous SCC of the head & neck can metastasize
- Most commonly to parotid lymph nodes
- SCC and melanoma from scalp,
auricle and face spread to their 1st order intra or periparotid nodes
- Aggressive disease with tendency to an infiltrative growth pattern and multiple recurrences [25]
- The appearance can vary from solid enhancing lesion to a necrotic mass
- In Australia,
due to the high prevalence of skin malignancy,
SCCs with parotid metastasis is common
- Nodal involvement plus parotid confers significantly worse prognosis compared to parotid metastasis alone [26]
- Patients with metastasis skin SCC involving the parotid gland had a high incidence of neck disease [27]
- Patients with clinical metastatic skin SCC should have CT/MRI/PET staging
Lung Adenocarcinoma Metastasis
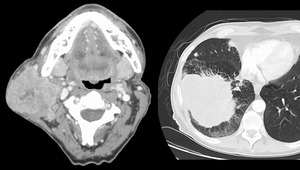
Fig. 38: Lung adenocarcinoma metastasis
57 year old male presented a large solid enhancing infiltrating parotid mass, involving mostly the superficial lobe, with extension towards the deep lobe.
Subsequent biopsy showed metastatic adenocarcinoma.
Further work up chest CT shows a large mass with lymphangiomatosis carcinomatosa.
References: University of Cincinnati Hospital Medical Center
B-cell Lymphoma with Parotid Nodal Involvement
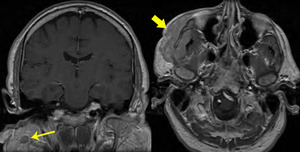
Fig. 39: B-cell lymphoma with parotid nodal involvement
55 year old female. T1 FS.
Large infiltrating mass over the right face extending deep to the right maxilla (large arrow).
Coronal post contrast T1 WI shows a well defined, hypoenhancing mass in the right parotid gland (small arrow).
Pathology showed B-cell lymphoma with parotid nodal involvement.
References: University of Cincinnati Hospital Medical Center
Angiosarcoma Metastasis
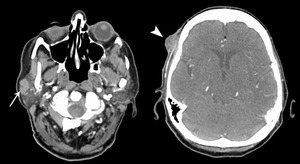
Fig. 40: Angiosarcoma metastasis
83 year old female. CT with contrast. Well defined enhancing superficial lobe mass (arrow) in a patient with an ipsilateral enhancing temporal scalp lesion (arrowhead).
References: University of Cincinnati Hospital Medical Center
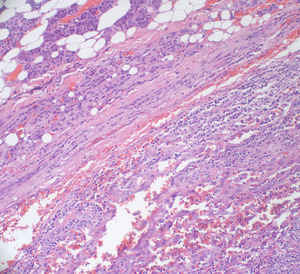
Fig. 41: Angiosarcoma metastasis
83 year old female. CT with contrast. Well defined enhancing superficial lobe mass (arrow) in a patient with an ipsilateral enhancing temporal scalp lesion (arrowhead).
References: University of Cincinnati Hospital Medical Center
- Angiosarcoma primarily arises in the skin or superficial soft tissue
- Vascular endothelial cell in origin
- Head & neck
- >60 years
- Local invasion with early lung metastasis
- Highly aggressive tumor [28]
- No reported case of angiosarcoma to the parotid in the literature (as of Aug 2013)
- Skin lesion may be hard to detect and even missed on PET [29]
Malignant Peripheral Nerve Sheath Tumor

Fig. 42: MPNST
Post contrast CT shows an ill defined, minimally enhancing hypodense tumor in the deep lobe of the right parotid.
References: University of Cincinnati Hospital Medical Center
- MPNST can arise from any organs of the head and neck.
- Strong association with NF1 (30-50%) and previous irradiation (4-11%) [30]
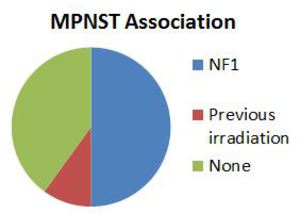
Fig. 43: MPNST associations
References: University of Cincinnati Hospital Medical Center
Melanoma Metastasis
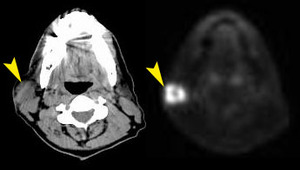
Fig. 44: Melanoma metastasis
55 year old male
PET/CT shows a large well-defined FDG-avid mass in the superficial lobe of the right parotid gland.
References: University of Cincinnati Hospital Medical Center
- Many have palpable lymph nodes at diagnosis (50%)
- Patients with metastatic melanoma to the parotid have worse prognosis compared to those from SCC [27]
- 5 year survival 40%,
mostly from distant metastatic disease
- Sentinel lymph node biopsy is advocated
Ethesioneuroblastoma Metastasis
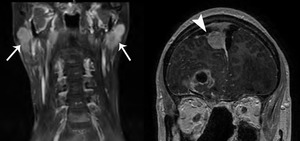
Fig. 45: Ethesioneuroblastoma metastasis
49 year old male. Symmetric ill-defined homogeneously enhancing bilateral parotid masses (arrows) in a patient with known ethesioneuroblastoma resected, metastasizing to the dura (arrowhead).
References: University of Cincinnati Hospital Medical Center
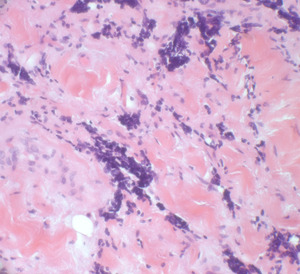
Fig. 46: Ethesioneuroblastoma metastasis
49 year old male. Symmetric ill-defined homogeneously enhancing bilateral parotid masses (arrows) in a patient with known ethesioneuroblastoma resected, metastasizing to the dura (arrowhead).
References: University of Cincinnati Hospital Medical Center
- Few cases reported [31]
- Small round blue tumor
- Arises from olfactory neuroepithelium
- Rare tumor: 1200 cases identified since 1924 in the literature
- 4 per 10 million
- Age: 3-90 years
- Varying degree of aggressiveness,
survival from a few months to 20 years [32]
Other
Hemangiopericytoma

Fig. 47: Hemangiopericytoma
42 year old female with a well-defined 3 cm homogeneously enhancing right parotid mass with some extension posterior and medial to the mandible.
References: University of Cincinnati Hospital Medical Center
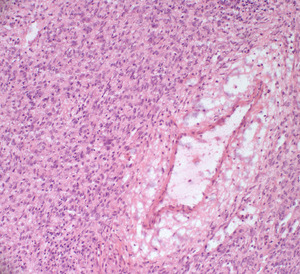
Fig. 48: A vessel with a “staghorn” configuration is surrounded by a syncytial sheet of epithelioid cells with eosinophilic cytoplasm
References: University of Cincinnati Hospital Medical Center
- Rare vascular tumor
- Can arise in any organ system,
most frequently skeletal muscle
- 30% in head & neck
- Spindle cell tumor
- Primarily in adults
- Painless mass
- Characteristically a very slow growing lesion and majority of the tumors are painless,
thus delay in presentation and diagnosis is a common feature
- Although imaging features non-specific,
thorough pre-operative imaging with CT/MRI is recommended [33]
Neuroendocrine Carcinoma
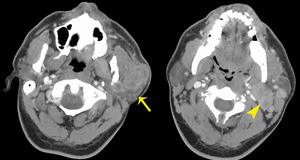
Fig. 49: Neuroendocrine carcinoma
47 year old male. CT with contrast.
Large infiltrating superficial lobe heterogeneously enhancing mass (arrow) extending into the deep lobe with lymphadenopathy (arrowhead).
References: University of Cincinnati Hospital Medical Center
- Primary salivary gland carcinoma with neuroendocrine differentiation is of rare occurrence,
especially so in the parotid gland,
reprsenting
- less than 1% of all carcinomas of parotid gland tumors.
- Report of acinic cell carcinoma with neuroendocrine differentiation has been published [34]

 T1 post contrast FS MRI (right) shows a fairly homogeneous enhancing mass (arrow) with hyperintense T2 signal and a well-defined low T2 signal capsule (arrowhead). References: University of Cincinnati Hospital Medical Center")
. The right parotid mass has deep lobe extension. References: University of Cincinnati Hospital Medical Center")
, involving both superficial and deep lobe of the left parotid, extending behind the angle of the mandible and across the anterior margin of the internal carotid artery. References: University of Cincinnati Hospital Medical Center")

 involving both the superficial and deep lobes of the right parotid. The carotid artery is displaced posteromedially (arrow) and has an ill-defined margin with the mass. References: University of Cincinnati Hospital Medical Center")
 centered in the left parotid, with abnormal ipsilateral nodes (arrowhead). References: University of Cincinnati Hospital Medical Center")

 in the right parotid gland that demonstrates irregular peripheral enhancement. The lesion is inseparable from the posterior aspect of the masseter muscle. The mass extends to the superficial skin with an irregular surface and deep into the retromandibular region. The overlying skin is ulcerated (arrowhead). There are necrotic ipsilateral neck lymph nodes (not shown). References: University of Cincinnati Hospital Medical Center")
 in the background. Note the intercellular bridges (small arrow & insert). References: University of Cincinnati Hospital Medical Center")
 and deep extension to the carotid sheath. References: University of Cincinnati Hospital Medical Center")




 and an enhancing solid nodule (arrowhead) in the superficial lobe of the left parotid gland. References: University of Cincinnati Hospital Medical Center")
 with effacement of the parapharyngeal space. The carotid sheath is displaced posteriorly. References: University of Cincinnati Hospital Medical Center")

 in both parotid glands in a patient with a history of scalp SCC. References: University of Cincinnati Hospital Medical Center")
 in the superficial lobe of the right parotid gland, extending to the skin. References: University of Cincinnati Hospital Medical Center")


.
Coronal post contrast T1 WI shows a well defined, hypoenhancing mass in the right parotid gland (small arrow).
Pathology showed B-cell lymphoma with parotid nodal involvement. References: University of Cincinnati Hospital Medical Center")
 in a patient with an ipsilateral enhancing temporal scalp lesion (arrowhead). References: University of Cincinnati Hospital Medical Center")


 in a patient with known ethesioneuroblastoma resected, metastasizing to the dura (arrowhead). References: University of Cincinnati Hospital Medical Center")

 extending into the deep lobe with lymphadenopathy (arrowhead). References: University of Cincinnati Hospital Medical Center")