Normal variants of the azygos system
Azygos continuation of the IVC
- Also known as absence of the hepatic segment of the IVC with azygos continuation
- The causative embryonic event is thought to be failure of formation of the right subcardinal–hepatic anastomosis with atrophy of the right subcardinal vein
- As a result,
blood is shunted from the suprasubcardinal anastomosis through an enlarged retrocrural azygos vein,
which is partially derived from the thoracic segment of the right supracardinal vein
- This was previously thought to be associated with severe congenital heart disease but is now recognized in asymptomatic patients
Further variants which result in abnormally enlarged retrocrural azygos and hemiazygos systems include:
- Duplication of the IVC with azygos and/or hemiazygos continuation
- Absence of the infrarenal portion of the IVC
It is important to be aware of these normal variants to avoid misdiagnosis of an enlarged retrocrural azygos system as adenopathy or a mass
Figure 8
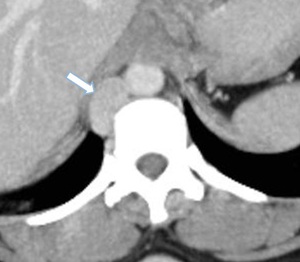
Fig.: Axial CT maximum intensity projection with IV contrast showing azygos continuation of the IVC. CT image reveals an abnormally dilated azygos vein (arrow).
Figure 9

Fig.: Coronal CT maximum intensity projection with IV contrast showing azygos continuation of the IVC (arrow)
Cisterna chyli and thoracic duct
Cisterna chyli
- The cisterna chyli is an elongated sac-like structure formed by the convergence of lymphatic channels
- It is situated under the right crus,
in front of the vertebral bodies of L1 and L2,
in between the aorta and azygos vein
Thoracic duct
- The thoracic duct commences at the superior aspect of the cisterna chyli at the level of T12
- It is situated between the aorta and the azygos vein
Figure 10

Fig.: Coronal HASTE MRI image shows the thoracic duct (curved arrow) that courses up the right side of the aorta from its origin at the cisterna chyli, which appears as a focal dilatation (arrow) in the retrocrural space.
Tubular structure inferior to the lower aspect of the cisterna chyli represents the afferent trunks (arrow head)
Pathology of the retrocrural space
Diaphragmatic crura
Primary malignancies affecting the diaphragmatic crura are rare
Metastatic deposits within the crura or retrocrural space occur via cephalic or caudal extension or local invasion from adjacent structure
- Lung
- Oesophageal
- Hepatic
- Renal
- Ovarian
- Lymphoma
Figure 11

Fig.: Axial contrast enhanced CT showing a subcentimetre benign lipoma (arrow) in the left crus
Figure 12
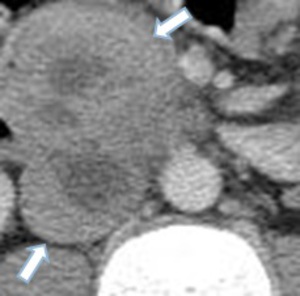
Fig.: Axial contrast enhanced CT with a large mass (arrows) invading the retrocrural space in a patient with metastatic renal cell carcinoma
Metastatic lesions
Malignancy is the most common cause of retrocrural lymphadenopathy
Figure 13

Fig.: Axial contrast enhanced CT with enlarged lymph nodes (arrow) in the retrocrural space in a patient with metastatic ovarian carcinoma
Inflammatory processes
Inflammatory conditions can result in a variety of abnormal retrocrural findings
Lymphadenopathy
- Pancreatitis
- Gastritis
- Amyloidosis
Ascites
Aortitis
- Inflammatory or infectious
Retroperitoneal fibrosis (Ormond’s disease)
- Chronic inflammatory condition characterized by the proliferation of fibrous tissue
Spondylosis deformans (bone spurs)
- Characterized by osteophyte formation on the anterolateral aspect of the vertebral bodies
- Usually right sided as aortic pulsations suppress their formation on the left
Figure 14

Fig.: Axial contrast enhanced CT with several small lymph nodes (arrow) in the retrocrural space in a patient with pancreatitis
Figure 15

Fig.: Axial contrast enhanced CT showing free fluid (arrow) in the retrocrural space in a patient with large volume ascites
Figure 16

Fig.: Axial contrast enhanced CT showing diffuse inflammation of the aorta (arrow) in a patient with giant cell arteritis
Figure 17
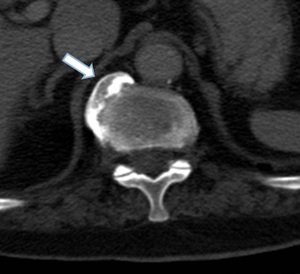
Fig.: Axial contrast enhanced CT demonstrating spondylosis deformans (arrow) on the right anterolateral aspect of T12 with displacement of the right crus
Vascular findings
Major aortic findings within the retrocrural space include:
- Suprarenal aneurysm
- Pseudoaneurysm
- Aortic rupture
- Aortic dissection
- Aortic haematoma
- Aortitis
Other vascular findings such as entrapment of renal artery by the diaphragmatic crus resulting in renal artery stenosis have been described
Figure 18

Fig.: Axial arterial phase CT shows an eccentric suprarenal aortic aneurysm (arrows) with partial thrombosis
Trauma related findings
Figure 19
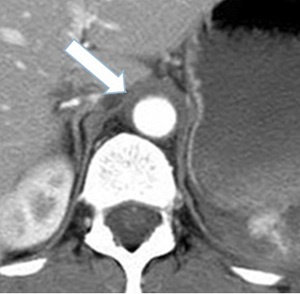
Fig.: Axial arterial phase CT in a patient with a peri-aortic haematoma (arrow) at the level of the diaphragmatic crura following a road traffic accident.
Similar findings are seen secondary to vertebral body or rib fractures
Retrocrural free air
This can be a difficult finding to distinguish given the relatively small area the retrocrural space occupies
Usually seen in relation to trauma resulting in either pneumo-thorax/mediastinum or pneumoperitoneum
Figure 20

Fig.: Axial CT depicting a small focus of retrocrural free air (arrow) following a penetrating thoracic injury
