ECR 2012 / C-0715
Radiological Study of the Orbit: What must the Radiologist see? CT and MRI Findings
This poster was previously presented in Spanish at the 2010 Congreso Nacional SERAM (A Coruña)
Congress:
ECR 2012
Poster Number:
C-0715
Type:
Scientific Exhibit
Keywords:
Head and neck, Eyes, Trauma, CT, MR, Ultrasound, Diagnostic procedure, Foreign bodies, Neoplasia
Authors:
M. A. Martin Perez1, J. M. Millán Juncos2, R. Blanco Hernández1, I. Martín García1, C. Martinez Lara1; 1Zamora/ES, 2Madrid/ES
DOI:
10.1594/ecr2012/C-0715
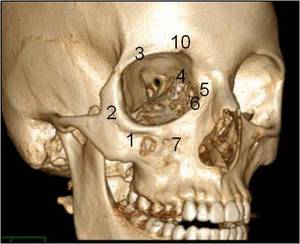
(3)
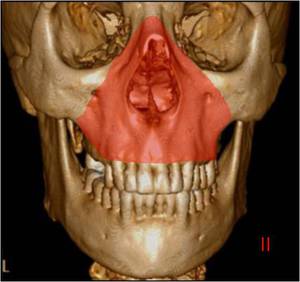
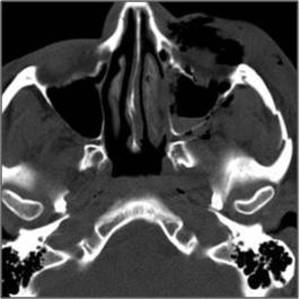
Supraorbital incisure (10)
Orbital plate of maxillary bone (1)
Zygomatic bone (2)
Infraorbital foramen (7)
Frontal process of maxillary bone (Anterior) (5)
Lacrimal bone (Posterior)(6)
Lamina papyracea of Ethmoid bone (4)")
Fig. 4:
Fig.4
Frontal bone (Orbital process)(3)
Supraorbital incisure (10)
Orbital...
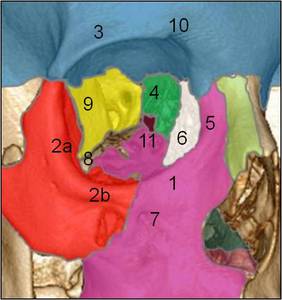
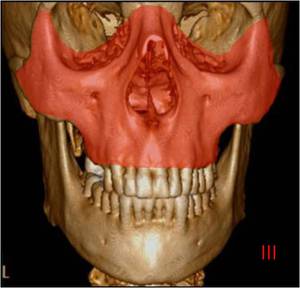
 (3)
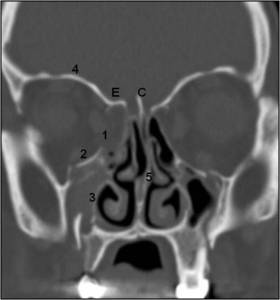
Lesser wing of sphenoid (9)
Supraorbital incisure (10)
Orbital plate of maxillary bone (1)
Maxillary process of zygomatic bone (2b)
Orbital process of palatinal bone (11)
Infraorbital foramen (7).
Inferior orbital fissure (8)
Frontal process of maxillary bone (Anterior) (5)
Lacrimal bone (Posterior)(6)
Lamina papyracea of Ethmoid bone (4)
Lateral aspect of spheniod body (9)
LATERAL WALL
- Orbital surface of zygomatic bone (2a)
- Frontal bone (3)
- Greater wing of sphenoid (9)")
Fig. 5:
Fig 5.
Frontal bone (Orbital process) (3)
Lesser wing of sphenoid...
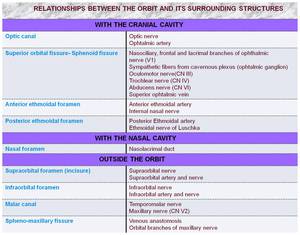
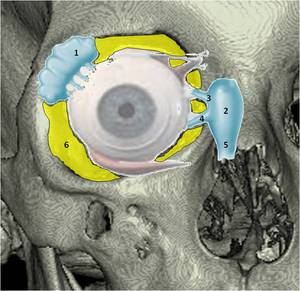
: Supraorbital artery and nerve
- Infraorbital foramen (5): Infraorbital artery and nerve
Inside the orbit:
- Optic canal (2): CN II and ophtalmic artery
- Superior orbital fissure (3): CN III, IV,V1, VI and superior ophtalmic vein.
- Inferior orbital fissure (4): CN V2 and inferior ophtalmic vein.")
Fig. 6:
Fig. 6.
- Supraorbital incisure (1): Supraorbital artery and nerve
-...

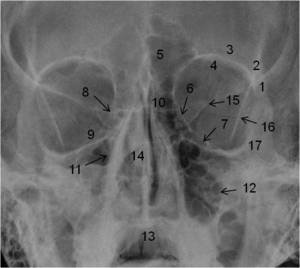
Fig. 7:
Fig. 7
Foramina and fissures of orbit. Relationships.

1. Zygomaticofrontal suture
2. Orbital process of frontal bone
3. Anterior orbital roof
4. Upper rim of orbit
5. Frontal sinus
6. Lamina papyracea
7. Posterior orbital floor
8. Posterior lacrimal crest
9. Anterior orbital wall
10. Frontal process of maxilla
11. Lateral nasal wall
12. Lateral maxillary wall
13. Hard palate
14. Perpendicular ethmoid plate and vomer
15. Superior orbital fissure
16. Oblique orbital line
17. Orbital process of zygoma")
Fig. 8:
Fig.8.
Frontal projection (Caldwell view)
1. Zygomaticofrontal suture
2....

Fig. 9:
Fig.9.
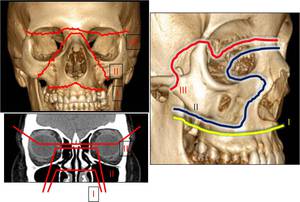
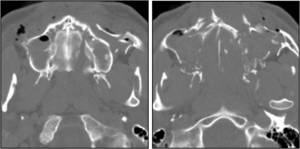
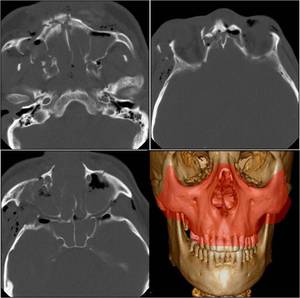
Orbital walls in a case of Lefort II fracture.
Reconstruction in the...

Fig. 10:
Fig.10.
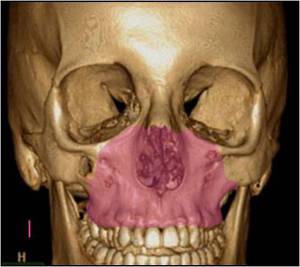
Le Fort fractures

Fig. 11:
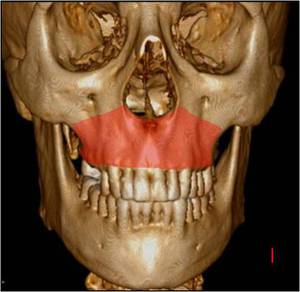
Fig.11.
Le Fort I Fracture, of Guerin or transverse fracture of the maxilla

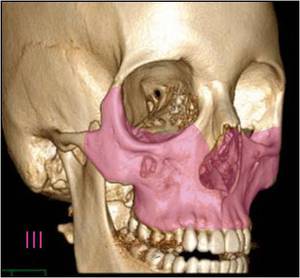
Fig. 12:
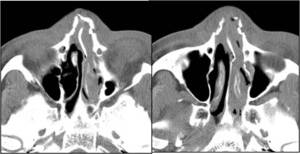
Fig.12.
Le Fort II or Pyramidal fracture

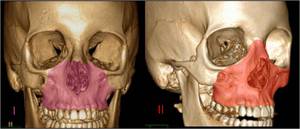
Fig. 13:
Fig.13.
Le Fort III or craniofacial disjunction

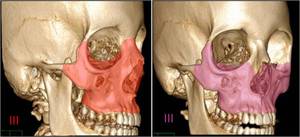
Fig. 14:
Fig.14.
Wassmund I fracture

Fig. 15:
Fig.15.
Wassmund III fracture

Fig. 16:
Fig.16.
Wassmund I and Le Fort II fractures comparison

Fig. 17:
Fig.17.
Wassmund III and Le Fort III fractures comparison

Fig. 18:
Fig.18.
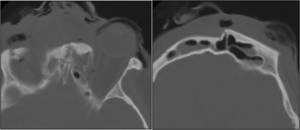
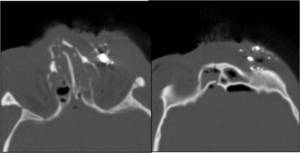
LeFort II fracture: comminuted fracture of maxillary sinus walls, with...

Fig. 19:
Fig.19.
LeFort III fracture or craniofacial disjunction:
The fracture line...

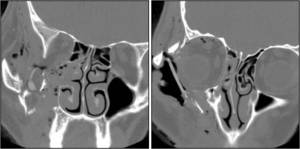
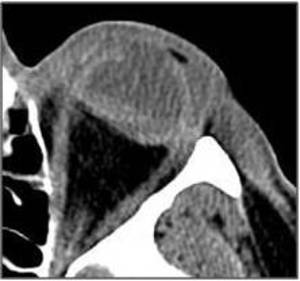
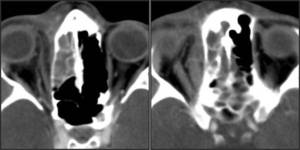
Fig. 20:
Fig.20.
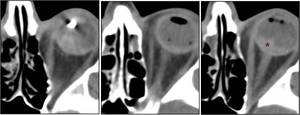
Orbital floor fracture with mild collapse, herniation of extraconic...

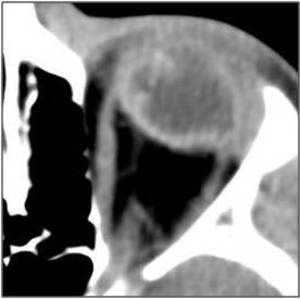
Fig. 21:
Fig.21.
Orbital floor collapse: CT Reconstructions in sagittal and coronal...

Fig. 22:
Fig.22.
Diplopia. Orbital floor fracture: Axial and Coronal CT images....

Fig. 23:
Fig.23.
Fracture-collapse of medial wall of the orbit: Lamina papyracea of...

Fig. 24:
Fig.24.
Diplopia. There is dislocation of the left medial rectus muscle in a...

Fig. 25:
Fig.25.
Nasal bone fracture and vertical lamina of maxillar-vomer: extending...

Fig. 26:
Fig.26.
Frontonasal and orbital collapse: Fracture of the anterior wall of the...

Fig. 27:
Fig.27.
Orbital apex fracture, and foreign bodies in soft tissues of the roof....

Fig. 28:
Fig.28.
Orbital "blow-out". Malar, lateral wall, medial wall and orbital floor...

Fig. 29:
Fig.29.
Orbitozygomatic comminuted fracture. Nasal bone, maxillary sinus...

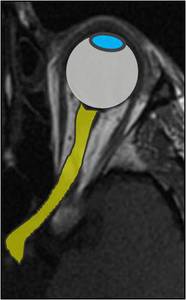
Fig. 30:
Fig.30.
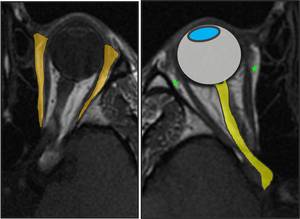
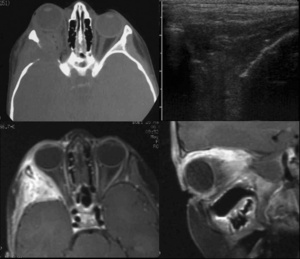
Illustration of the section; Eyeball and optic nerve.
Modified...

Fig. 31:
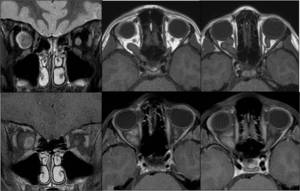
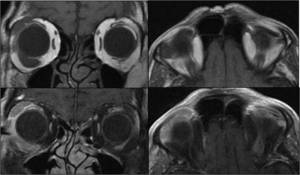
Fig.31.
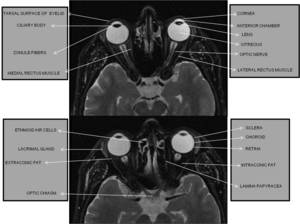
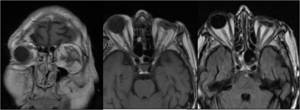
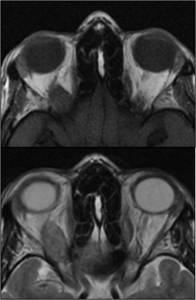
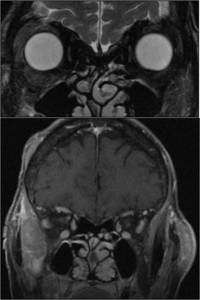
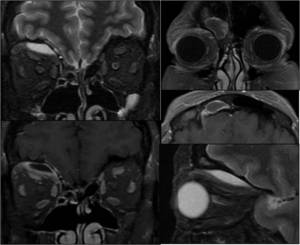
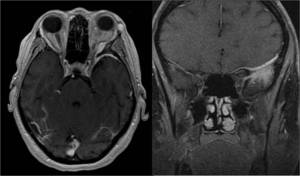
MRI anatomy I

Fig. 32:
Fig.32.
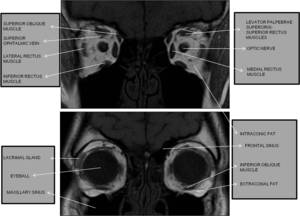
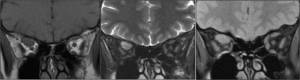
MRI Anatomy II

Fig. 33:
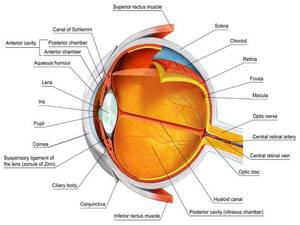
Eyeball anatomy

Fig. 34:
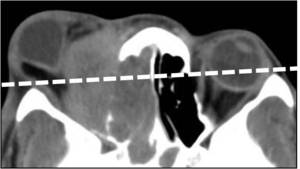
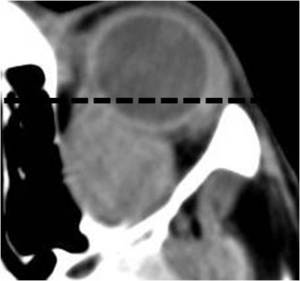
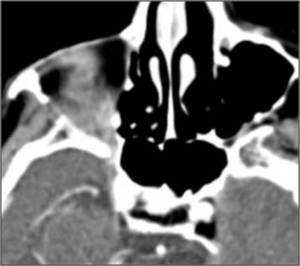
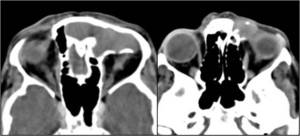
Fig.34.
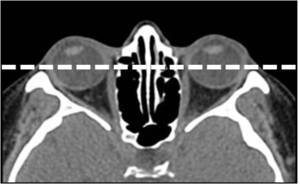
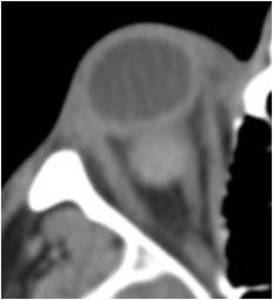
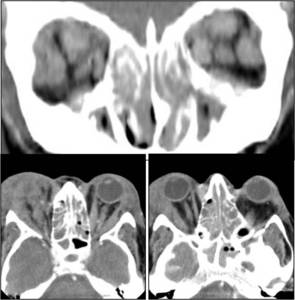
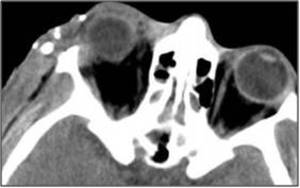
Axial CT scan. Normal eyeball position

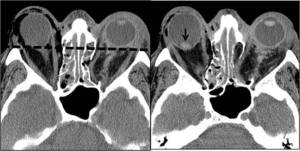
Fig. 35:
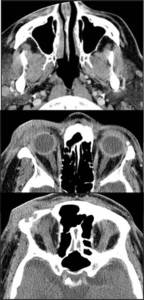
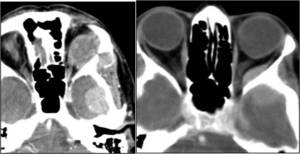
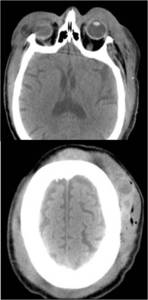
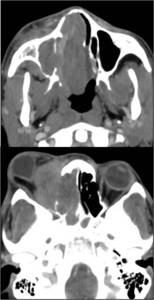
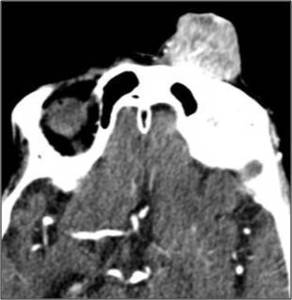
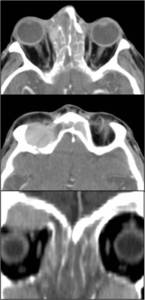
Fig.35.
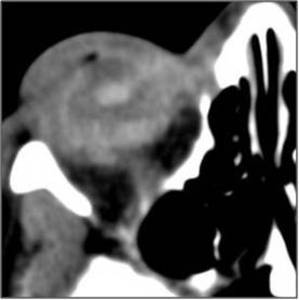
Great right unilateral exophthalmos due to nasal and intraorbital...

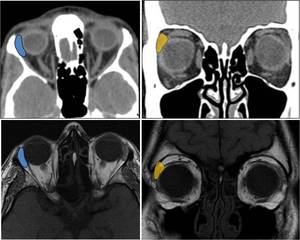
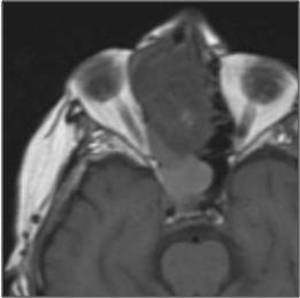
Fig. 36:
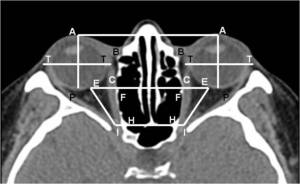
Fig.36.
Modified outline in axial CT scan from Mafee et Al

Fig. 37:
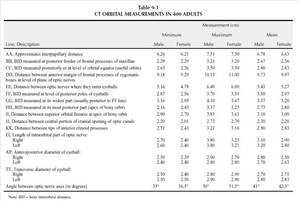
Fig.37.
Table from Mafee MF. Pruzansky S. Corrales MM. et at. Evaluation of...

Fig. 38:
Fig.38.
Intralenticular foreign body: Metal shrapnel

Fig. 39:
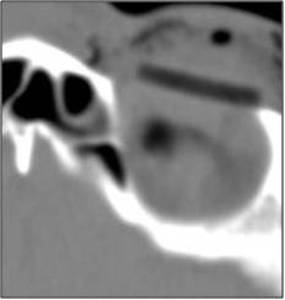
Fig.39.
Left eyeball deformity produced by vegetable foreign body not...

Fig. 40:
Fig.40.
Intraocular foreign body: Splinter of wood. Intraconic, extraconic and...
.")
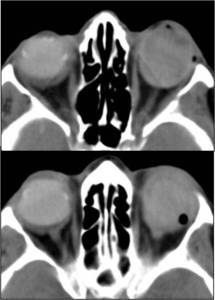
Fig. 41:
Fig.41.
Axial CT scan. Ocular perforation. Metallic foreign...

Fig. 43:
Fig.43.
Facial trauma. Perforation of the left eye. Loss of volume....

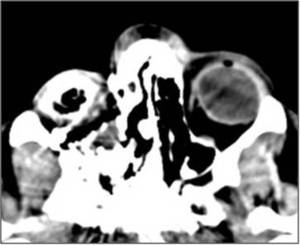
Fig. 44:
Fig.44.
Traumatic injury of right orbit. Blow-out of the eyeball with...
. Trauma against a doorknob. Haematoma and extraconic air")
Fig. 45:
Fig.45.
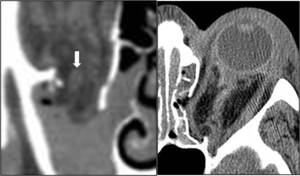
Eyeball disruption (arrow). Trauma against a...

Fig. 46:
Fig.46.
Ocular fracture due to a golfball impact. Vitreous hemorrhage...

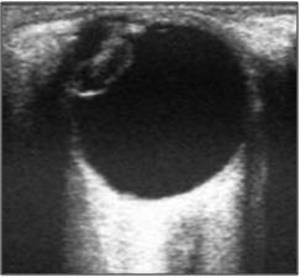
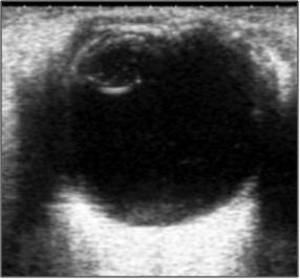
Fig. 47:
Fig.47.
Ophthalmic ultrasound. Traumatic cataract. Hyperechogenic...
. Extraconic haematoma and left medial rectus muscle herniation. Right periconic air.")
Fig. 48:
Fig.48.
Orbital fracture; Both medial...

Fig. 49:
Fig.49.
Preseptal haematoma and traumatic lens luxation.

Fig. 50:
Fig.50.
Barotrauma. Blow-out with ocular emptying. Lack of eyeball.
. Hemorrhage in the left eyelid and extraconic air presence.")
Fig. 51:
Fig.51.
Anticoagulated patient. Conjunctival hemorrhage in the right eye....

Fig. 52:
Fig.52.
Sintrom treatment. Expulsive hemorrhage in the right eye.

Fig. 53:
Fig.53.
Volume loss and bleeding in left vitreous body after cataract...

Fig. 54:
Metal worker. Retroocular fragment of metal in conic fat. Vitreous...

Fig. 55:
Fig.55.
Ophthalmic ultrasound. Cataract. Increased volume of the...

Fig. 56:
Fig.56.
Right eye ocular prosthesis

Fig. 57:
Fig.57.
T1WI in coronal and axial planes and T2 FLAIR WI. History of left...

Fig. 58:
Fig.58.
Phthisis bulbi.
Right eyeball atrophy, with abnormal morphology...

Fig. 59:
Fig.59.
Left eyeball prosthesis.

Fig. 60:
Fig.60.
CT without and after intravenous contrast media...
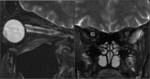
Fig. 61:
Fig.61.
MRI T2WI. Optic neuritis.
Swollen appearance with foci of...

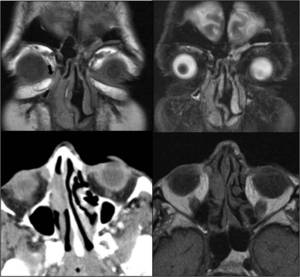
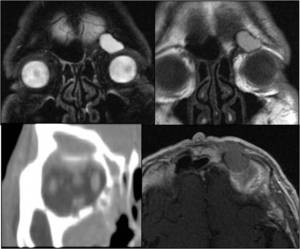
Fig. 62:
Fig.62.
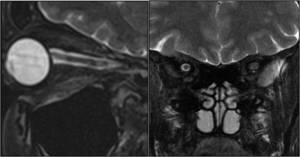
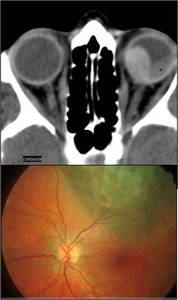
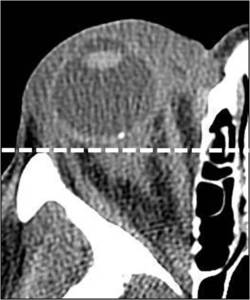
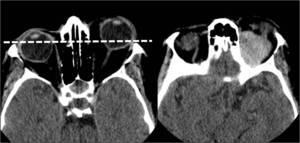
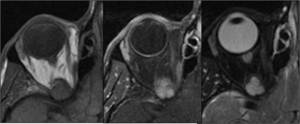
Choroidal melanoma with episcleral extension. CT and eye fundus...
 and after contrast media administration (2). T1WI (3), T2WI (4 and 8) and T1WI after gadolinium administration (5, 6 and 7). High density is observed in the precontrast CT scan and discrete enhancement at MRI. Paucimelanotic lesion. The tumor is typically hyperintense on T1WI by the melanic pigment and moderately hypointense on T2WI.")
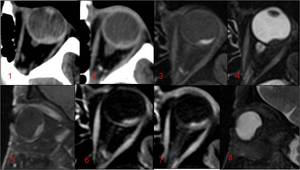
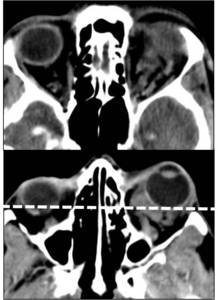
Fig. 63:
Fig.63.
Choroidal Melanoma: TC without (1) and after contrast media...

Fig. 64:
Fig.64.
Optic nerve sheath meningioma-en-plaque.
Right...

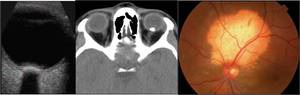
Fig. 65:
Fig.65.
Choroidal osteoma.
Ophthalmic ultrasound, which...
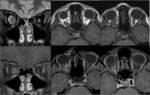
Fig. 66:
Fig.66.
Neurofibromatosis type I. Right optic nerve glioma. Coronal MRI: ...
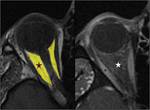
Fig. 67:
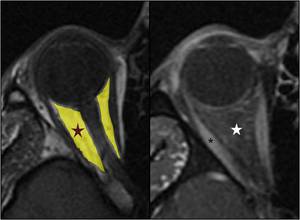
Fig.67.
Illustration of intraconal space.
Intraconal Space (Star) limited...
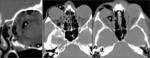
Fig. 68:
Fig.68.
Trauma. Right orbital floor fracture with eyelid edema and...
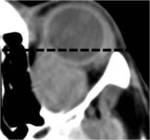
Fig. 69:
Fig.69.
Idiopathic inflammatory pseudotumor.
“Myositic...

Fig. 70:
Fig.70.
Lamina papyracea fracture-collapse with conjunctival chemosis, and...
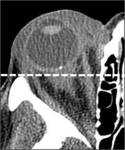
Fig. 71:
Fig.71.
Craniofacial trauma.
Intraconal and preseptal hematoma.
It is...

Fig. 72:
Fig.72.
Fibrinolysis for pulmonary embolism. Developments in 6 hours...

Fig. 73:
Fig.73.
Intraorbital venous angioma: tortuous vessels cluster in...

Fig. 74:
Fig.74.
Sudden proptosis and chemosis in right eye....
 after gadolinium contrast media administration.")
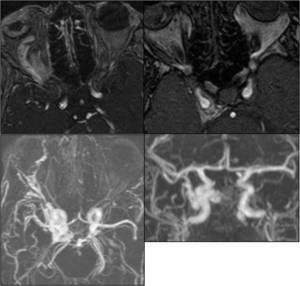
Fig. 75:
Fig.75.
Vitreous hemorrhage. Right Carotid cavernous fistula.
3D TOF...

Fig. 76:
Fig.76.
Melanoma. Temporal bleeding.
Left exophthalmos. Ophthalmic veins...

Fig. 77:
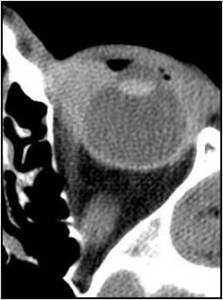
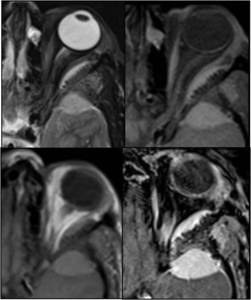
Fig.77.
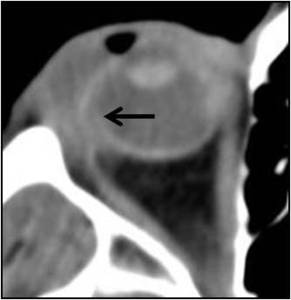
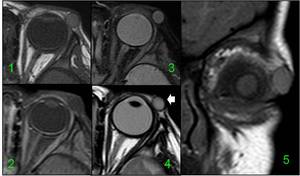
Cavernous hemangioma. CT after contrast media administration. Conal...
 and T2WI in axial plane. Rounded homogenous well defined mass in the conal fat. It is isointense to muscle on T1WI and hyperintense on T2WI with homogeneous enhancement.")
Fig. 78:
Fig.78.
Cavernous hemangioma. T1-weighted MR images (without and after...
; axial and sagittal planes")
Fig. 79:
Fig.79.
Orbital lymphoma.
Invasion of conal fat by multiple similar to...
 and T2WI.
Paucimelanotic melanoma.
Slightly hyperintense on T1WI and T2WI compared to muscle lesion. Incomplete hemosiderotic ring and enhancement after gadolinium administration.")
Fig. 80:
Fig.80.
Metastases from melanoma.
T1-weighted images, 3DFSPGR...
.")
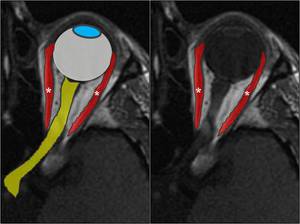
Fig. 81:
Fig.81.
Graphic of the section.
Extraocular muscles (asterisk).

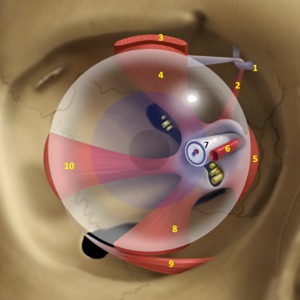
Fig. 82:
Fig.82.
Extraocular muscles. Frontal view.
1.TROCHLEA
2.SUPERIOR OBLIQUE...

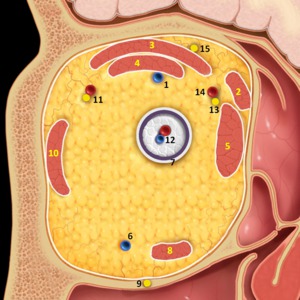
Fig. 83:
Fig.83.
Extraocular muscles. Coronal section.
1.SUPERIOR OPHTALMIC...

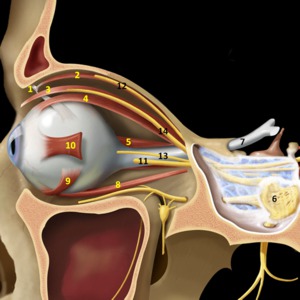
Fig. 84:
Fig.84.
Extraocular muscles. Sagittal view.
1.TROCHLEA
2.SUPERIOR OBLIQUE...

Fig. 85:
Fig.85.
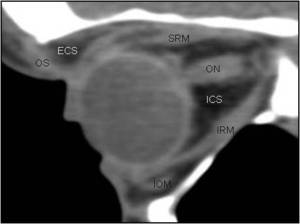
CT of the orbit. Sagittal reconstruction. Anatomy.
OS. Orbital...

Fig. 86:
Fig.86.
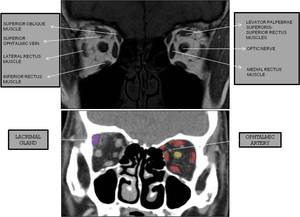
Extraocular muscles. MRI and CT correlation.
Coronal plane

Fig. 87:
Fig.87.
Extraocular muscles. MRI and CT correlation.
Coronal and axial planes

Fig. 88:
Fig.88.
Extraocular muscles. MRI correlation. Axial and coronal planes

Fig. 89:
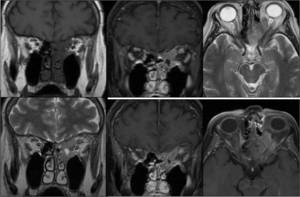
Fig.89.
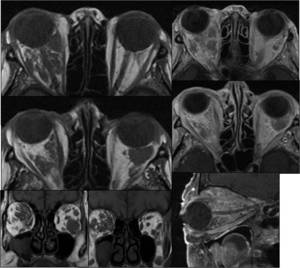
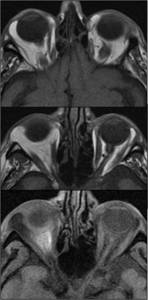
Grave's disease: T1WI and T2WI in axial plane.
Thyroid...

Fig. 90:
Fig.90.
Grave's disease: T1WI and T1-T2WI with fat saturation in coronal...

Fig. 91:
Fig.91.
Order of likelihood of muscle involvement in thyroid...
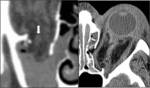
Fig. 92:
Fig.92.
Extraocular muscles.Traumatic injury. (See floor and medial wall...

Fig. 93:
Fig.93.
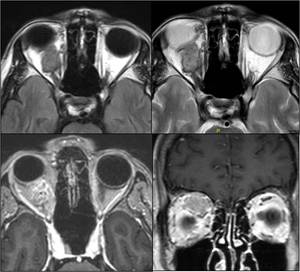
Inflammatory diffuse thickening in right orbit. Relatively homogeneous...
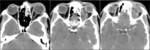
Fig. 94:
Fig.94.
Idiopathic orbital pseudotumor-Myositic orbital pseudotumor....

Fig. 95:
Fig.95.
Lymphoma...
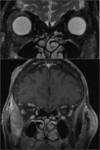
Fig. 96:
Fig.96.
Lymphoma with extraocular muscle involvement.
T2WI and T1WI after...

Fig. 97:
Fig.97.
Frontal mucocele with orbital extension....
.")
Fig. 98:
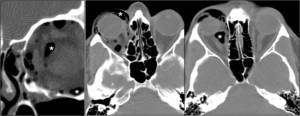
Fig.98.
Graphic of the section.
Extraconal space(asterisk).

Fig. 99:
Fig.99.
Extraconal space. Frontal graphic. Content.
1. LACRIMAL GLAND
2....

Fig. 100:
Fig.100.
Lacrimal gland. CT and MR Images.

Fig. 101:
Fig.101.
Retroseptal cellulitis.
Orbital edema with chemosis after nasal...

Fig. 102:
Fig.102.
Several cases of extraconic air presence after...

Fig. 103:
Fig.103.
Palpebral hematoma over the orbital septum and...

Fig. 104:
Fig.104.
Nonspecific lacrimal swelling. At 15 days, parotid enlargement...

Fig. 105:
Fig.105.
Cellulitis-infectious myositis....
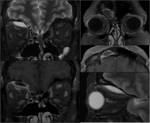
Fig. 106:
Fig.106.
Wegener's Disease.
Frontal sinusitis (right). T2WI and T1 after...

Fig. 107:
Fig.107.
Lacrimal Idiopathic Pseudotumor....
 in axial and coronal planes. See the well-defined oval mass occupying extraconal and palpebral fat ahead of Tenon's fascia. Homogeneous appearance, no infiltration, and higher signal than muscle..
T1WI with fat saturation (2).
PDWI with FATSAT (3) and T2WI (4). High signal in both, and loss of signal in T1WI with saturation of fat.")
Fig. 108:
Fig.108.
Dermoid cyst: T1WI (1 and 5) in axial and coronal planes. See the...

Fig. 109:
Fig.109.
Lipoma of orbit.
T1WI and T1WI with fat saturation. Increased volume...

Fig. 110:
Fig.110.
Left: extraaxial metastasis of prostate carcinoma with orbital...

Fig. 111:
Fig.111.
Lymphoma B of orbit: Invasion of ethmoid sinus and superior orbital...

Fig. 112:
Fig.112.
Eye rupture secondary to suicide attempt. View bone fragments...

Fig. 113:
Fig.113.
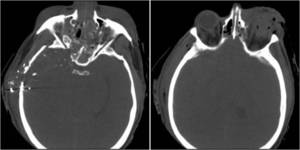
Facial and orbital hematoma for aggression. Trimalar...

Fig. 114:
Fig.114.
Fragments of glass on right orbital region with proptosis and...

Fig. 115:
Fig.115.
Subgaleal hematoma with orbital soft tissue extension and to the...
, and after gadolinium contrast media administration.")
Fig. 116:
Fig.116.
Alar Meningioma: spread en-plaque.
MRI with T1-weighted images and...

Fig. 117:
Fig.117.
Alar Meningioma: spread en plaque.
MRI with T1-weighted images with...

Fig. 118:
Fig.118.
Squamous cell carcinoma of maxilla. Extension to skull base, nose...

Fig. 119:
Fig.119.
Nasal...

Fig. 120:
Fig.120.
Orbitofrontal cutaneous squamous cell carcinoma...
")
Fig. 121:
Fig.121.
Nasal plasmacytoma with orbital extension to lacrimal sac (arrow)

Fig. 122:
Fig.122.
Solitary fibrous tumor of nasal cavity: orbital extension. Erosion...

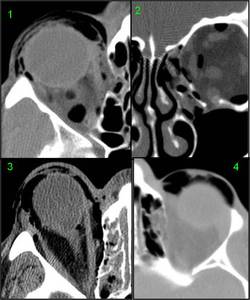
Fig. 123:
Fig.123.
Frontal mucocele with mass effect over the orbital roof

Fig. 124:
Fig.124.
Frontal mucocele with extension to orbital apex.
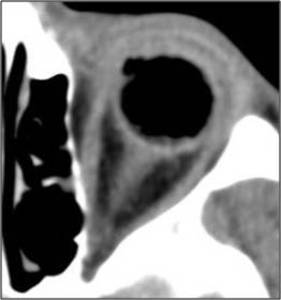
 and metal from the rim in the periorbital soft tissues (black arrows).")
Fig. 42:
Fig.42.
Ocular trauma caused by the bursting of a tire. Rubber fragments are...

Fig. 125:
Fig.125.
Frontal mucocele. History of polyposis. Rupture of frontal sinus...

Fig. 126:
Fig.126.
Recurrence of squamous cell carcinoma in orbit in a patient...
 show retrobulbar mass, proptosis and erosion of the
external orbit wall (lesser wing of sphenoid). Axial and sagittal enhanced T1WI show enhancing soft tissue mass filling the pterion, temporal fossa, left lesser sphenoid wing and extraconal space.")
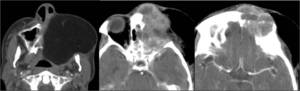
Fig. 127:
Fig.127.
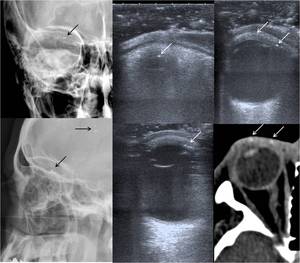
Eosinophilic granuloma . US and axial CT through the orbit
(bone...