Clinically suspicious lesions referred for imaging should first be evaluated with mammography.
In patients with questionable findings at mammography and with lesions that are difficult to access with mammography,
they should be characterized additionally by ultrasonography (US).
US can be useful in demonstrating the cystic nature of a lesion and for examination of axillary region which proves helpful for staging.
Male Breast Anatomy
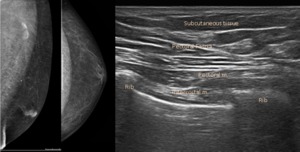
Fig. 1: Normal appearance of the male breast. The normal male breast contains predominantly subcutaneous adipose tissue, a few rudimentary ductal tissue beneath the nipple and a prominent pectoralis major muscle. The appearance is similar to that of the prepubertal girl. Because of the need for progesterone for lobular development, genetically normal men do not develop lobules as the ligaments Cooper and do not develop the lesions that occur in this lobule. Therefore, fibrocystic changes and lobular carcinomas do not occur in genetically normal men.
Diseases in the male breast can affect the skin and subcutaneous tissues,
stroma/glandular elements,
neurovascular and lymphatic structures.
Skin and Subcutaneous Tissues
Epidermal inclusion cysts or sebaceous cysts
Epidermal inclusion cysts and sebaceous cysts typically present as intradermal,
partially dermal lesions or lesions in the subcutaneous tissue,
witch results from the obstruction of the pilous folicule.
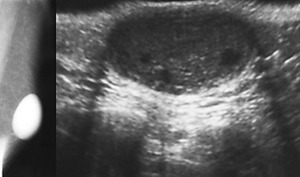
Fig. 2: Epidermal inclusion cyst. Mammography and US show a round, circumscribed superficial mass. On US, they can be homogeneous or heterogeneous in echotexture and usually are hypoechoic. Often show the “claw” sign, a sonographic feature where the skin is compressed posteriorly and an echogenic curvilinear line from the skin is seen posteriorly along with posterior acoustic enhancement. In some cases, a “tail” extends into the subcutaneous tissue, which is indicative of a dilated neck of the sebaceous gland. If rupture occurs, the subsequent inflammatory reaction can be difficult to differentiate from malignancy on imaging.
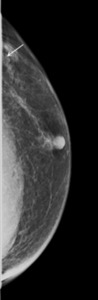
Fig. 3: Skin lesion projected on the external quadrants on craniocaudal (CC) mammogram. It appears as a nodular density surrounded by a radiolucent halo formed by the air trapped in the interface between the elevated lesion and the skin during compression.
Hematoma
On mammography,
hematomas are radiopaque,
are circumscribed or irregular,
and can be difficult to distinguish from malignancy.
A history of trauma,
anticoagulant use,
or a clotting disorder are important on differentiation.
On US,
acute hematomas typically are hyperechoic,
but are variable in appearance over time,
often becoming more hypoechoic.
Lipoma
Lipomas are common,
benign,
fat-containing neoplasms that may occur singly,
or may be numerous as occurs in multiple lipomatosis.
They can occur in any fat-containing region of the body and not uncommonly occur in the breast.
These lesions slow growing and present as soft,
well-circumscribed lumps in the subcutaneous tissues.
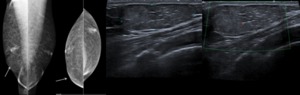
Fig. 4: Breast lipoma. A 35-year-old man presented with a soft lump in the rigth breast. Mammography shows a thin capsule which surrounds radiolucent lipomatous tissue. Calcification in lipomas occurs only rarely, possibly due to focal areas of fat necrosis. US demonstrates a well-circumscribed solid lesion with an homogenous internal echo pattern, often with capsule and hyperechoic horizontal internal septations as in this patient. They may appear hyper- or isoechoic to the surrounding fat. There is no associated significant distal acoustic shadowing or distortion of the surrounding breast tissue.
Fat Necrosis
Fat necrosis of the breast in both sexes is usually associated with trauma,
most commonly secondary to biopsy or surgery.
The mammographic appearances of fat necrosis can vary from those of a well-circumscribed mass of homogeneous fat density to an irregular spiculated density/ hypoechoic mass,
that may be difficult to differentiate radiologically from a carcinoma.
Architectural distortion,
skin thickening,
retraction or dystrophic calcifications are also present.
Stromal and Glandular Elements
Gynecomastia
Gynecomastia is defined as an abnormal increase in the stromal and ductal components of the male breast.
It occurs most commonly in adolescent boys and in men older than 50 years.
The condition represents about 85% of breast masses in men.
It manifests clinically as a soft,
mobile,
tender mass in the retroareolar region.
The condition may be unilateral or bilateral and frequently asymmetric.
It may appear as triangular or flame-shaped density/hypoechoic area behind nipple,
mild prominence of the subareolar ducts or diffuse ductal enlargement or even to a homogeneously increase of density of the breast having the appearance of that of a young woman.
Three mammographic patterns of gynecomastia have been described: nodular,
dendritic,
and diffuse.
|
Etiologies of gynecomastia
|
|
(a) hormonal -related to an hormone imbalance with a relative excess of estradiol levels than testosterone levels or to dysfunction of the adrenal,
thyroid,
or pituitary glands
(b) systemic - cirrhosis,
chronic renal failure with hemodialysis,
chronic obstructive pulmonary disease,
and tuberculosis
(c) drug induced - secondary to exogenous estrogens,
digitalis,
cimetidine,
omeprazole,
spironolactone,
thiazides,
digoxin,
ergotamine,
tricyclic antidepressants,
androstenedione,
anabolic steroids,
and antiandrogens and gonadotropin-releasing hormone analogs,
highly active antiretroviral therapy to treat HIV and marijuana.
(d) tumors - particularly of testicular,
pituitary,
and adrenal origin or secondary to hepatomas or lung cancers
(e) idiopathic
|
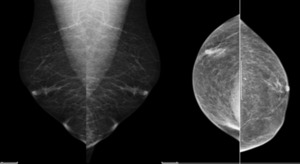
Fig. 5: Pseudogynaecomastia in the obese is due to the accumulation of fatty tissue which is easily differentiated from true gynecomastia by mamography. This typically demonstrates an enlarged breast filled with radiolucent fat only.
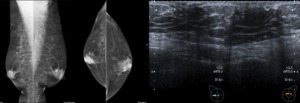
Fig. 6: Bilateral gynecomastia in a 47-year-old man: left and right views of mammography and US demonstrate triangular or flame-shaped densities/hypoechoic areas in both subareolar areas.
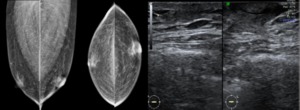
Fig. 7: Asymmetric gynecomastia in a 52-year-old man. The findings are slight more prominent in the left breast than in the right.
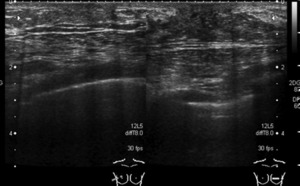
Fig. 8: Unilateral gynecomastia in a 60-year-old man with a tender left breast mass. US show a triangular hypoechoic area behind the left nipple.US may be helpful in questionable cases as it depicts normal-appearing ductal structures and no mass.
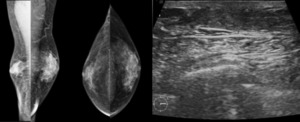
Fig. 9: Asymmetric gynecomastia. A 63-year-old man presented a bilateral breast enlargement. Left and right lateral oblique (LO) and CC views demonstrate a diffuse no-homogeneous increase of density of the breast concentric to the nipple, which occupies much of the left breast., and partially right breast, that radiate out in a fan as would be expected for the distribution of the ducts. US demonstrates an triangular area of diffuse hypoechogenicity in the subareolar region concentric to the nipple, consistent with gynaecomastia.
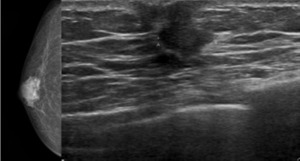
Fig. 10: Nodular gynecomastia in a 50-year-old man presented with a rubbery lump in the left breast, that corresponds to unilateral gynecomastia with nodular configuration. Rarely, diagnostic difficulties may arise in distinguishing between early carcinoma and early focal gynecomastia, as both are hypoechoic as in this patient. The most important radiographic features used to differentiate an area of gynecomastia from malignancy are those of a mass with a concentric subareolar position, absence of a spiculated margin, no calcifications and no secondary signs of malignancy such as changes due to overlying skin involvement.
Mastitis With or Without Abscess
Mastitis is an infection of the breast tissue that can be complicated by abscess formation.
On mammography mastitis often presents with unilateral breast enlargement with skin and trabecular thickening.
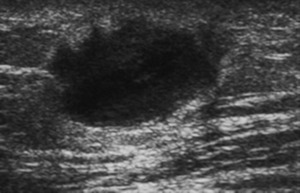
Fig. 11: Abscess in a 53-year-old man presented with a dolorous in left breast lump. US shows an irregular mass predominantly anechoic with internal echoes, wide and irregular wall associated a thickening skin.
Pseudoangiomatous Stromal Hyperplasia
Pseudoangiomatous Stromal Hyperplasia rarely presents as a localized mass,
and more commonly is found incidentally on histology of breast biopsy specimens performed for other indications.
It can be circumscribed or partially circumscribed on mammography and ultrasound.
Carcinoma
Breast cancer in men is most common after the age of 60.
In comparison with women,
men have a higher median age at diagnosis,
and are more likely to have lymph node involvement,
have a more advanced stage at diagnosis,
and have tumors positive for estrogen and progesterone receptors.
|
Risk factors of male breast cancer
|
|
advanced age
positive family history
Jewish origin
black race
altered estrogen metabolism
exogenous estrogens
infectious orchitis
Klinefelter syndrome
radiation to the chest
BRCA2 mutations (hereditary breast cancers)
|
Imaging of the male breast cancer is similar to that found in women.
It can have a variety of appearances,
including well defined,
ill-defined,
spiculated dense/hypoechoic mass,
non-parallel to the skin.
The lesions may be round,
oval,
or irregular and are frequently lobulated.
Sound transmission is variable and can range from dense distal acoustic shadowing to acoustic enhancement.
Microcalcifications can occur and.
tend to be large,
round and scattered,
rather than grouped.
A discrete mass at mammography or US is suspicious for malignancy.
An eccentric location relatively to the nipple is highly suspicious for cancer.
Secondary signs,
such,
nipple retraction,
skin ulceration or thickening,
increased breast trabeculation,
and axillary adenopathy,
occur earlier in male patients because of smaller breast size.
At pathologic analysis,
cystic lesions commonly demonstrate malignant findings; therefore,
all cysts and complex masses should be worked up as potentially malignant lesions.
Benign conditions that may mimic male breast cancer include gynecomastia,
lipoma,
epidermal inclusion cyst,
pseudoangiomatous stromal hyperplasia,
and intraductal papilloma.
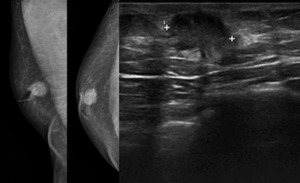
Fig. 12: Ductal carcinoma. A 67-year-old man presented with a lump in the rigth breast. LO and CC mammograms and US of the right breast demonstrate an irregular spiculated opacity/ hypoechoic with skin thickening and nipple retraction.
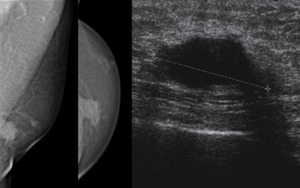
Fig. 13: Ductal carcinoma. A 72-year-old man presented with a lump in the left breast. LO and CC mammograms and US of the left breast demonstrate an irregular, ill-defined heterogeneous opacity/ hypoechoic mass distant from the nipple and overlying the pectoralis muscle.
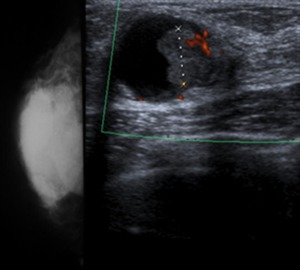
Fig. 14: 57-year-old man with palpable mass in rigth retroareolar breast. CC view shows irregular mass in rigth breast. US reveals heterogeneous mass with edge shadowing containing nodular component. The pathologic analysis revealed a papillary ductal carcinoma in situ.
Neoplasms in the breast can originate from the neurovascular and lymphatic structures,
such lymphoma,
neuromas,
schwannomas,
and glomus tumors,
although these neoplasms are uncommon in both women and men.
Men may also present with metastasis to the breast from nonbreast primary malignancies.
Other rare tumors include myofibroblastoma,
low-grade spindle cell sarcoma,
and inflammatory pseudotumor.
