A monocentric retrospective study was conducted including all patients (five) operated with confirmed pathological diagnosis of ACC with pre-operative imaging (CT and/or MRI) from 1996 to 2012.
Twenty successive patients with resected BD-IPMN without malignant transformation and with pre-operative MRI were also included in a “control group”.
The study was approved by our local institutional review board and patient consent was waived.
Cases
Five patients (four women and one man),
26 to 59 years old at diagnosis were included.
Twenty successive patients (eleven women and nine men),
25 to 79 years old,
operated between 2005 and 2008,
with pathological diagnosis of BD-IPMN were retrospectively selected.
Surgery was performed for acute pancreatitis in eleven patients (55%),
suspicion of intracystic nodule in two cases (10%),
size increase in one patient (5%),
suspicion of main duct (MD) involvement in one patient (5%) and size of cyst above 3 cm in five patients (25%).
Data collection
Clinical and biological data were extracted from medical records for cases and controls.
Clinical follow up was recorded from 1 to 11 years (mean: 6.25 years) in ACC group.
Histopathological characterization
One pathologist analyzed retrospectively the 5 specimens fixed in 4% formaldehyde and embedded in paraffin and confirmed the diagnosis of ACC using the previously described criteria (3).
The diagnostic of BD-IPMN was also confirmed by histological examination.
Branch ducts were screened to confirm the presence of a papillary and mucinous lesion.
The exclusion criteria were main duct lesion and the presence of an adenocarcinoma (even micro-infiltrating).
The ACC specimens were analyzed at the gross and histopathological levels (fig.
3) to identify features,
specific of ACC (not or rarely found in BD-IPMN), which may be seen on common radiological examination.
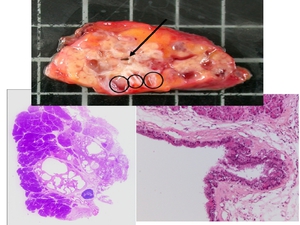
Fig. 3: Gross and histopathological level in pathology of ACC
Imaging methods
- Patients with ACC: computed tomography (CT) were available for all and magnetic resonance imaging (MRI) for all but one.
CT scans were performed with and without contrast-medium intra-venous injection.
MRI was performed with at least T1 and with T2-weighted sequences in axial plane.
Three patients underwent magnetic resonance cholangiopancreatography (MRCP).
- Patients with BD IPMN: MRI with the same protocol as ACC,
including MRCP were available for all within one year delay before surgery (according to inclusion and exclusion criteria).
Imaging analysis
The following radiological features,
based on radio-pathological confrontation and knowledge of BD-IPMN characteristics,
were studied independently by two radiologists: number of cysts recorded as < or ≥ 5,
size of the biggest cyst,
shape of cyst (round or elongated),
distribution in pancreas (head,
uncinate process,
isthmus,
body and tail),
pattern defined as “close peripheral small cysts” (i.e.
: numerous small cysts present in a small portion of parenchyma and in peripheral location),
presence of calcification,
communication with main pancreatic duct and diameter of the main pancreatic duct.
Statistical analysis
The clinical,
histological and imaging characteristics of the 2 populations were first recorded,
and then compared using two-tailed tests and p values < 0.15 were considered statistically significant.
Then,
the clinical and imaging characteristics of patients with ACC and with BD-IPMN were compared in univariate analyses using the chi-square test or Fisher’s exact test,
as appropriate.
All variables associated with a ACC diagnosis in univariate analysis with p values <0.15 were used to build a simple-to-use score for predicting the diagnosis of ACC.
Sensitivity and specificity values of the different cut-off levels of the score were calculated.

