ECR 2013 / C-1245
The initial and long-term results of endovascular treatment of subclavian and innominate artery lesions in UKC Maribor
Congress:
ECR 2013
Poster Number:
C-1245
Type:
Scientific Exhibit
Keywords:
Vascular, Interventional vascular, Arteries / Aorta, MR-Angiography, CT-Angiography, Catheter arteriography, Stents, Recanalisation, Angioplasty, Obstruction / Occlusion, Dilatation
Authors:
B. Polanec1, S. Breznik2, A. Slanič3, J. Lučev3, J. Matela3; 1Pesnica/SI, 2Pernica /SI, 3Maribor/SI
DOI:
10.1594/ecr2013/C-1245
. References: Radiology department, UKC Maribor - Maribor/SI")
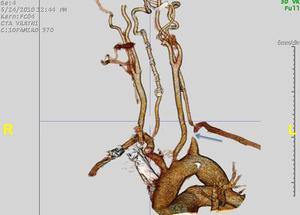
Fig. 1:
CTA before procedure shows lesion of left subclavian artery (arrow).

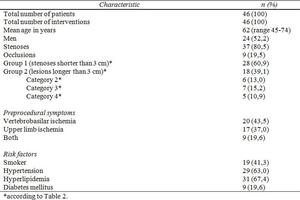
Table 1:
Patients characteristics.
). References: Radiology department, UKC Maribor - Maribor/SI")
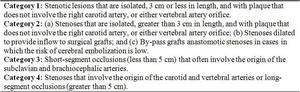
Table 2:
Classification of the subclavian artery and innominate artery lesions (from...

Table 3:
Procedural data for 46 interventions.
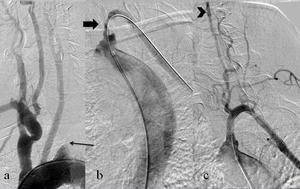
 of left subclavian artery (a). After antegrade recanalization with hydrophilic guidewire and predilatation (thick arrow) (b) stent was placed and antegrade vertebral flow achieved (arrowhead)(c). References: Radiology department, UKC Maribor - Maribor/SI")
Fig. 2:
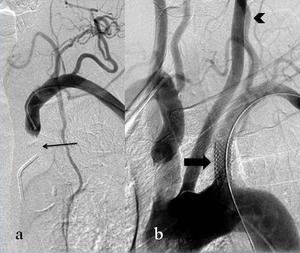
Aortic arch angiography showed occlusion (thin arrow) of left subclavian artery...
 retrograde attempt was made via brachial artery (a). Excellent technical success, including antegrade vertebral flow (arrowhead), was achieved after stent placement (thick arrow) (b). References: Radiology department, UKC Maribor - Maribor/SI")
Fig. 3:
In case of unsuccesful antegrade recanalization (thin arrow) retrograde attempt...