ECR 2013 / C-1349

Endometrial carcinoma: Diagnostic strategy by using advanced MR techniques
Congress:
ECR 2013
Poster Number:
C-1349
Type:
Educational Exhibit
Keywords:
Genital / Reproductive system female, MR, MR-Diffusion/Perfusion, MR-Spectroscopy, Diagnostic procedure, Cancer
Authors:
M. Takeuchi, K. Matsuzaki, M. Harada; Tokushima/JP
DOI:
10.1594/ecr2013/C-1349

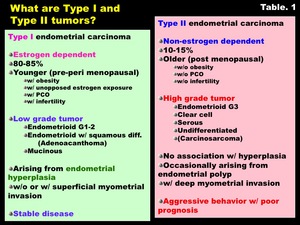
Table 1:
What are Type I and Type II tumors?

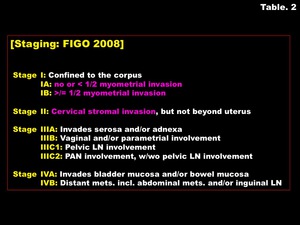
Table 2:
Staging: FIGO 2008

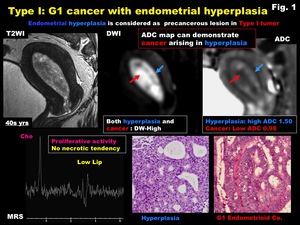
Fig. 1:
Type I: G1 cancer with endometrial hyperplasia

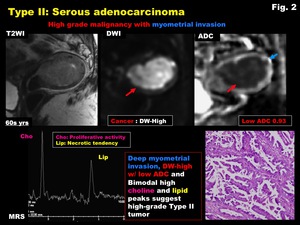
Fig. 2:
Type II: Serous adenocarcinoma

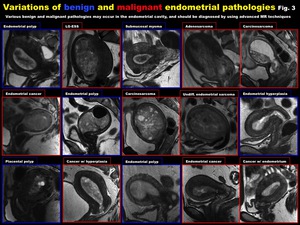
Fig. 3:
Variations of benign and malignant endometrial pathologies

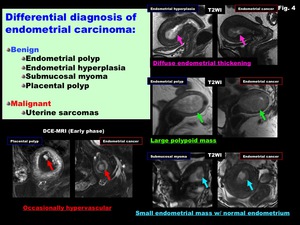
Fig. 4:
Differential diagnosis of endometrial carcinoma

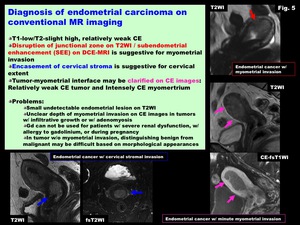
Fig. 5:
Diagnosis of endometrial carcinoma on conventional MR imaging

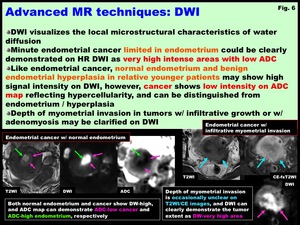
Fig. 6:
Advanced MR techniques: DWI
 Advanced MR techniques: DWI")
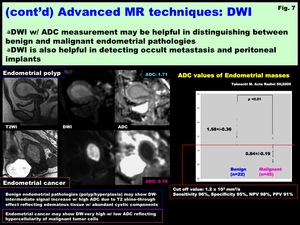
Fig. 7:
(cont’d) Advanced MR techniques: DWI

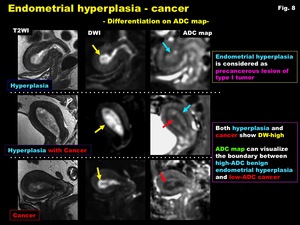
Fig. 8:
Endometrial hyperplasia - cancer
-Differentiation on ADC map-
 with normal endometrium
-Differentiation on ADC map-")
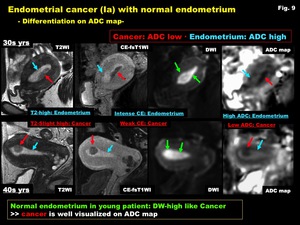
Fig. 9:
Endometrial cancer (Ia) with normal endometrium
-Differentiation on ADC map-

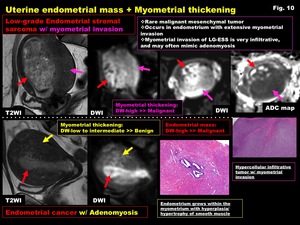
Fig. 10:
Uterine endometrial mass + Myometrial thickening

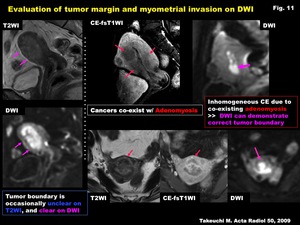
Fig. 11:
Evaluation of tumor margin and myometrial invasion on DWI

Fig. 12:
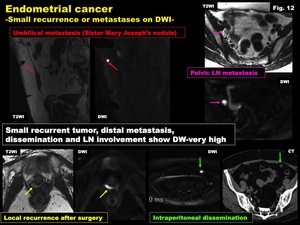
Endometrial cancer
-Small recurrence or metastases on DWI-

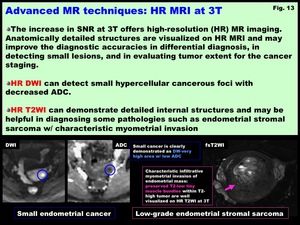
Fig. 13:
Advanced MR techniques: HR MRI at 3T

-Small lesions-")
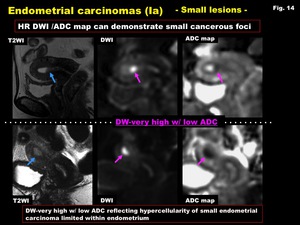
Fig. 14:
Endometrial carcinomas (Ia)
-Small lesions-

-Small lesions-")
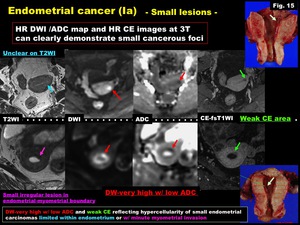
Fig. 15:
Endometrial cancer (Ia)
-Small lesions-

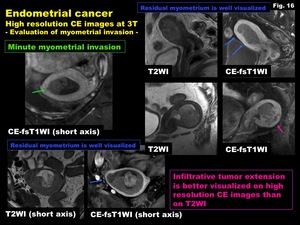
Fig. 16:
Endometrial cancer
High resolution CE images at 3T
-Evaluation of myometrial...

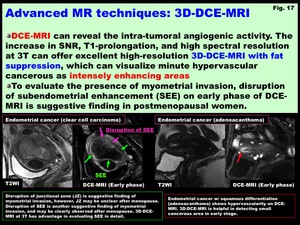
Fig. 17:
Advanced MR techniques: 3D-DCE-MRI

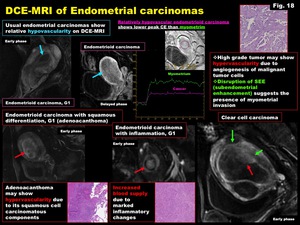
Fig. 18:
DCE-MRI of Endometrial carcinomas
")
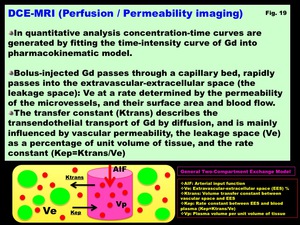
Fig. 19:
DCE-MRI (Perfusion / Permeability imaging)

-Clinical applications-")
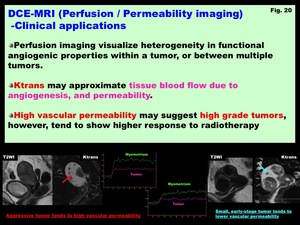
Fig. 20:
DCE-MRI (Perfusion / Permeability imaging)
-Clinical applications-
 of Endometrial cancer")
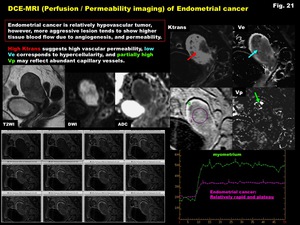
Fig. 21:
DCE-MRI (Perfusion / Permeability imaging) of Endometrial cancer

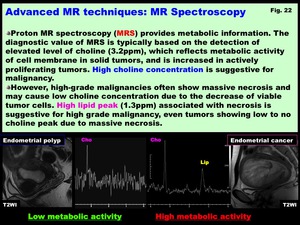
Fig. 22:
Advanced MR techniques: MR Spectroscopy

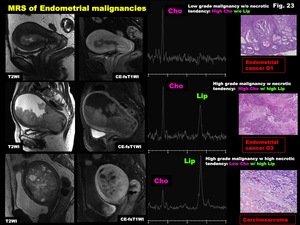
Fig. 23:
MRS of Endometrial malignancies

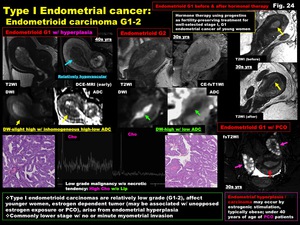
Fig. 24:
Type I Endometrial cancer:
Endometrioid carcinoma G1-2

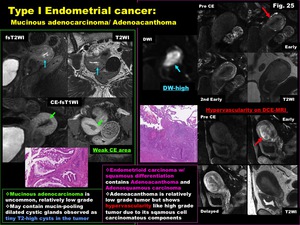
Fig. 25:
Type I Endometrial cancer:
Mucinous adenocarcinoma/ Adenoacanthoma

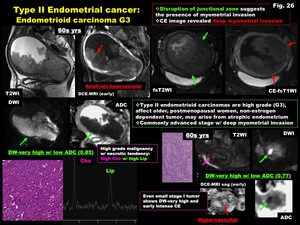
Fig. 26:
Type II Endometrial cancer:
Endometrioid carcinoma G3

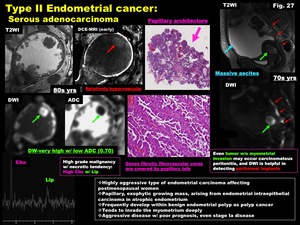
Fig. 27:
Type II Endometrial cancer:
Serous adenocarcinoma

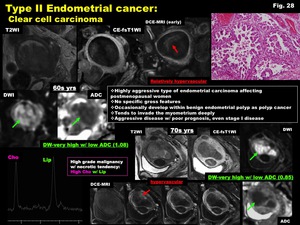
Fig. 28:
Type II Endometrial cancer:
Clear cell carcinoma

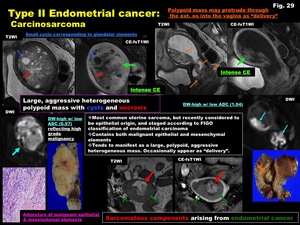
Fig. 29:
Type II Endometrial cancer:
Carcinosarcoma

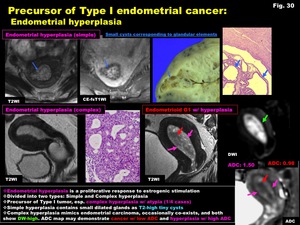
Fig. 30:
Precursor of Type I endometrial cancer:
Endometrial hyperplasia

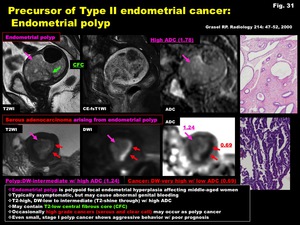
Fig. 31:
Precursor of Type II endometrial cancer:
Endometrial polyp
")
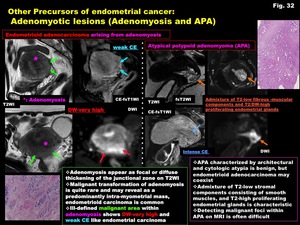
Fig. 32:
Other Precursors of endometrial cancer:
Adenomyotic lesions (Adenomyosis and...