Type:
Educational Exhibit
Keywords:
Neoplasia, Metastases, Cancer, Imaging sequences, Contrast agent-intravenous, Ablation procedures, MR-Functional imaging, MR, CT, Liver, Interventional non-vascular, Abdomen
Authors:
D. K. Filippiadis, M. Mademli, A. Mazioti, N. Oikonomopoulos, S. Argentos, A. D. Kelekis, N. L. Kelekis; Athens/GR
DOI:
10.1594/ecr2013/C-1376
Background
Hepatocellular carcinoma is the sixth most common cancer type and the third most common cause of cancer-related death.
Hepatic metastases are the most common liver tumors; liver is the most common site of metastasis,
second only to lymph nodes.
Due to the hepatic anatomy and perfusion,
metastasis can originate from any primary tumor; however most common sites of origin include colon,
breast,
lung and pancreas.
Image-guided tumor ablation provides curative treatment in properly selected patients or appropriate therapeutic options whenever surgical techniques are precluded.
Whenever liver is concerned the two most common thermal ablation techniques used are radiofrequency (RFA) and microwave (MWA) ablation.
During MWA,
tissues are heated faster than with radiofrequencies due to the more efficient transfer of heat.
In contrast to radiofrequencies the circulation of which is hindered by high tissue impedance,
microwaves can penetrate and thus heat any kind of tissue.
Furthermore,
microwaves are confined close to the antenna as opposed to radiofrequency which during ablation flows through the body to reach the grounding pads.
Microwaves are governed by higher heating efficiency than radiofrequency which renders them unaffected by “heat sink” effect and blood vessels resulting in larger ablation volumes achieved in less time.

Fig. 2: CT-guided RFA of HCC. Both foci were ablated by means of an umbrella-shaped radiofrequency electrode in the same session.
References: 2nd Radiology Dpt, University General Hospital "ATTIKON"
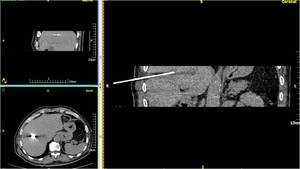
Fig. 3: CT-guided MWA of two metastatic foci in the liver from bronchogenic carcinoma. MPR images (both parallel and perpendicular to the needle axis) provide valuable information upon penetration depth, exact position of the antenna in relation to the target and its margins and to essential close by anatomic structures.
References: 2nd Radiology Dpt, University General Hospital "ATTIKON"
Tumor response assessment post ablation is important in determining treatment success and future therapy.
Initially,
tumor response was assessed on the basis of the World Health Organization (WHO) criteria and the Response Evaluation Criteria in Solid Tumors (RECIST).
Both WHO and RECIST criteria appreciate tumor response on the basis of determining changes in tumor and its anatomic size therefore they address tumor response on the basis of tumor shrinkage.
Recently mRECIST criteria were proposed for which image acquisition protocols optimization and consistency in the same protocol throughout follow-up examinations are requisites.
Similarly to RECIST assessment of overall response with mRECIST includes evaluation of the response of both target and nontarget lesions as well as potential new lesions.
However,
concerning the assessment of target lesion's response,
mRECIST appreciate apart from size reduction,
the intratumoral arterial enhancement as viable tumor tissue.


 provide valuable information upon penetration depth, exact position of the antenna in relation to the target and its margins and to essential close by anatomic structures. References: 2nd Radiology Dpt, University General Hospital "ATTIKON"")