Immediately post ablation session,
a Computed Tomography scan including (non-contrast,
arterial and portal phase) of the upper abdomen (from lung base to right kidney level) should be performed in order to identify (and possibly treat) any potential complications (eg pneumothorax,
hemorrhage etc.)
After patient's discharge from the hospital a common follow-up strategy for assessment of tumor response includes contrast enhanced multiphasic (non-contrast,
arterial,
portal,
delayed phases) imaging with Computed Tomography or Magnetic Resonance at 1st and then every 3 months post ablation session.
Total ablation of a hepatic lesion appears in CT as a homogeneous non-enhancing attenuation at the site of the ablated volume.
Usually gas can be seen in the immediate post-session scan which in most cases resolves until the 1 month follow-up scan.
Evidence of tumor remnants or recurrence include residual or new areas of contrast enhancement either marginal or internally to the ablation zone.
KEEP IN MIND:
Fibrous tissue due to scarring enhances with a slow and persistent mode throughout arterial,
portal and delayed phase as opposed to tumor remnants or recurences which illustrate arterial enhancement and portal/delayed wash-out.

Fig. 4: Upper row: noncontrast (1A), arterial (1B) and portal (1C)phase of enhancement immediate post microwave ablation of a metastatic hepatic lesion (colon adenocarcinoma).
Lower row (same patient): noncontrast (2A), arterial (2B) and portal (2C)phase of enhancement 1 month post microwave ablation.
Immediately post ablation there inner enhancement in the ablated zone. One month post ablation there is a significant decrease of the surrounding reactive inflammation and still there is no inner enhancement in the ablated zone.
These findings constitute with successful outcome of the interventional procedure.
References: 2nd Radiology Dpt, University General Hospital "ATTIKON"
MRI (conventional T1WI,
T2WI,
dynamic contrast-enhanced imaging),
for tumor response assessment post liver thermal ablation,
is considered the most accurate method in early detection of residual/recurrent tumors.
In MRI,
total ablation of a hepatic lesion appears as an area of high signal intensity in T1-weighted sequences with homogeneous lack of Gadolinium enhancement.
Residual or reccurent tumor is governed by imaging findings similar to the tumor appearance prior to the ablation.
One disadvantage of MRI is its incapability to distinguish viable cells from reactive granulation tissue.
KEEP IN MIND:
Functional imaging,
including diffusion MR imaging and apparent diffusion coefficient (ADC) mapping,
has the ability to provide unique insight about molecular water distribution within a tumor,
and therefore indicate tumor viability degree at cellular level.
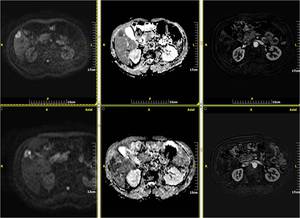
Fig. 5: Metastatic lesion from bronchogenic carcinoma. MRI showing restricted diffusion on DWI and ADC map (1a,b) and early enhancement of the lesion in arterial phase of the dynamic study after subtraction (1c).
Follow-up MRI one month after treatment with RadioFrequency Ablation(RFA): high signal in DWI corresponds to T2 “sign through” effect and not in restricted diffussion(2a,b). Also there is no enhancement of the lesion, with only faint linear perilesional enhancement due to post RF hyperemia in arterial phase of the dynamic study after subtraction (2c).
These findings constitute with successful outcome of the interventional procedure.
References: 2nd Radiology Dpt, University General Hospital "ATTIKON"

Fig. 6: Follow-up MRI of the same patient 17 months post RF ablation showing increased SI in T2WI (1a), restricted diffusion (1b,c), low SI in THRIVE(2a), early contrast enhancement in arterial phase (2b) and wash out in delayed enhancement phase(10min)(2c). These findings constitute with local recurrence.
References: 2nd Radiology Dpt, University General Hospital "ATTIKON"

Fig. 7: HCC after MW ablation demonstrates residual tumor as high signal intensity lesion in T2WI(1a) low SI in THRIVE, early enhancement in arterial phase of the dynamic study after subtraction (1c) and wash out in delayed enhancement phase(1H)(1d). in contrast to the above findings the successfully ablated area shows high SI in THRIVE(1b) and no enhancement in arterial phase of the dynamic study after subtraction (1c).
References: 2nd Radiology Dpt, University General Hospital "ATTIKON"
Contrast-enhanced ultrasound (CEUS) can provide valuable information and assess tumor response faster and at lower cost than computed tomography or magnetic resonance imaging.
KEEP IN MIND:
One disadvantage is that CEUS cannot be used in order to examine the total liver parenchyma for disease progression as CT and MR imaging can.

Fig. 8: A: HCC post RFA. Contrast enhanced ultrasound one month post ablation session illustrates enhancement of the residual tumor at arterial (A) phase and wash-out at delayed (B) phase. On the other hand, the ablated tumor illustrates no contrast uptake in both arterial and delayed phase.
References: K. Chatzimixail, Lecturer of Diagnostic Radiology, 2nd Radiology Dpt, University General Hospital
Recently,
fluorodeoxyglucose positron emission tomography - computed tomography (PET-CT) imaging is increasingly used for tumor response and therapy appreciation post ablation.
Residual or recurrent tumor demonstrates significantly higher standardizied values of uptake than the ones of reactive inflammation at the ablation margin.
PET-CT uses a functional agent for tumor assessment with potentially earlier detection of residual or recurrent tumor.
KEEP IN MIND:
False-negative results of PET-CT have been reported in lesions with a diameter < 1cm due to partial volume effects and in patients suffering from diabetes.
False-positive results of PET-CT have been reported in patients suffering from hepatic abscess.

, arterial (1B) and portal (1C)phase of enhancement immediate post microwave ablation of a metastatic hepatic lesion (colon adenocarcinoma).
Lower row (same patient): noncontrast (2A), arterial (2B) and portal (2C)phase of enhancement 1 month post microwave ablation.
Immediately post ablation there inner enhancement in the ablated zone. One month post ablation there is a significant decrease of the surrounding reactive inflammation and still there is no inner enhancement in the ablated zone.
These findings constitute with successful outcome of the interventional procedure. References: 2nd Radiology Dpt, University General Hospital "ATTIKON"")
 and early enhancement of the lesion in arterial phase of the dynamic study after subtraction (1c).
Follow-up MRI one month after treatment with RadioFrequency Ablation(RFA): high signal in DWI corresponds to T2 “sign through” effect and not in restricted diffussion(2a,b). Also there is no enhancement of the lesion, with only faint linear perilesional enhancement due to post RF hyperemia in arterial phase of the dynamic study after subtraction (2c).
These findings constitute with successful outcome of the interventional procedure. References: 2nd Radiology Dpt, University General Hospital "ATTIKON"")
, restricted diffusion (1b,c), low SI in THRIVE(2a), early contrast enhancement in arterial phase (2b) and wash out in delayed enhancement phase(10min)(2c). These findings constitute with local recurrence. References: 2nd Radiology Dpt, University General Hospital "ATTIKON"")
 low SI in THRIVE, early enhancement in arterial phase of the dynamic study after subtraction (1c) and wash out in delayed enhancement phase(1H)(1d). in contrast to the above findings the successfully ablated area shows high SI in THRIVE(1b) and no enhancement in arterial phase of the dynamic study after subtraction (1c). References: 2nd Radiology Dpt, University General Hospital "ATTIKON"")
 phase and wash-out at delayed (B) phase. On the other hand, the ablated tumor illustrates no contrast uptake in both arterial and delayed phase. References: K. Chatzimixail, Lecturer of Diagnostic Radiology, 2nd Radiology Dpt, University General Hospital")