Keywords:
Kidney, Contrast agents, CT, Contrast agent-intravenous, Transplantation
Authors:
J. M. Gutiérrez, M. C. Sebastia, B. Miquel, L. Buñesch, L. Peri, C. Nicolau; Barcelona/ES
DOI:
10.1594/ecr2013/C-1555
Methods and Materials
During 2010,
20 non-diabetic patients with renal insufficiency (IV-V) (15 men and 5 women; 32-77 years,
mean 53) underwent an angio-CT scan one month before the living-donor renal transplantation.
All the patients were informed about all aspects of this clinical trial and they signed an informed consent form.
In our series,
the leading causes of chronic renal failure were polycystic kidney disease (3 patients),
IgA-associated glomerulonephritis (3 patients),
ischemic nephropathy (2 patients) and hypertension (2 patients).
Table 1 shows the causes of renal failure in each patient.
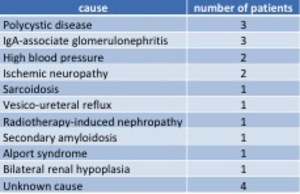
Fig. 1: Table 1. Causes of chronic renal failure.
In all cases,
CIN prophylactic measures involved saline hydration and administration of n-acetylcysteine and sodium bicarbonate following the regimen described next.
The day before the angioCT scan,
patients received 1200 mg of NAC every 12 hrs and a nonsteroidal anti-inflammatory drug.
On the day of the procedure,
patients were administered 1200 mg of NAC every 12 hrs and sodium bicarbonate 3mg/kg,
an hour before the study.
In addition,
patients received intravenous hydration with isotonic saline solution (0.45%).
On average,
patients were administered 671 cc (two thirds after the test) (Fig.
1).
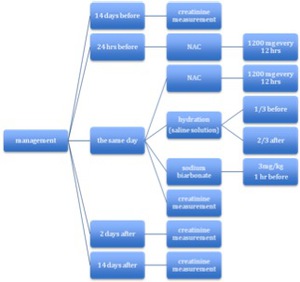
Fig. 2: Figure 1. Diagram showing the management schedule of patients
The radiological contrast agent was Iopromide (300 mg/ml),
a hyposmolar non-ionic monomer.
100 ml of Iopromide and 40 ml of saline solution were injected at 40 ml/s.
The creatinine levels were measured 15 days before and immediately before the angio-CT and 2 days after and 15 days after the angio-CT study.
We also evaluated the dialysis requirements of the patients before the renal transplant.
