ECR 2013 / C-2010
Diagnostic yield of Digital Breast Tomosynthesis vs Digital Mammography in the assessment of breast cancer: a study on surgical specimens.
Congress:
ECR 2013
Poster Number:
C-2010
Type:
Scientific Exhibit
Keywords:
Breast, Mammography, Surgery, Neoplasia
Authors:
C. Molinari1, A. Gualano1, E. Di Gaetano1, V. Londero1, R. Girometti1, S. Vecchio2, A. Taibi3, C. Zuiani1, M. Bazzocchi1; 1Udine/IT, 2Bologna/IT, 3Ferrara/IT
DOI:
10.1594/ecr2013/C-2010
.")
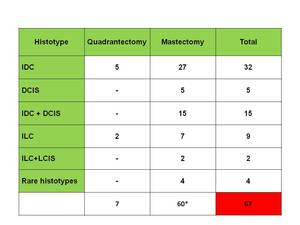
Table 1:
Lesions found at the histopathological analysis of the specimens. All the...

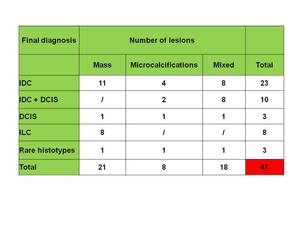
Table 2:
Lesions correctly found with both DBT and DM. DBT and DM recognized 47...

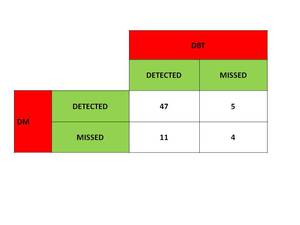
Table 3:
Malignantl esions correctly recognized with DBT and DM. As you can see DBT and...
 of a 60 years-old woman treated for a IDC confirmed at histhopatological analysis. Readers missed the lesion with DM (A), but with DBT (B) they found the lesion as a spiculated mass (C).")
Fig. 3:
Surgical specimen (mastectomy) of a 60 years-old woman treated for a IDC...

Fig. 4:
Plot of the detectability scores of DBT and DM. DBT showed signifcantly higher...
 of a 53 years-old woman with a IDC confirmed at hysthology. The readers gave a score of 4 to DM (A) and 5 to DBT (B). With DBT the margins were better seen and judge as fully visible (arrow).")
Fig. 5:
Surgical specimen (quadrantectomy) of a 53 years-old woman with a IDC confirmed...