We ask what pathologies can be found at the periphery of the orbits in imaging and how can we achieve accurate diagnosis. First step to correct diagnosis of these entities is profound knowledge of orbital anatomy in CT and MRI.
Most helpful is the differentiation of four orbital compartments: ocular,
conal,
intra- and extraconal compartment.
Location of a lesion to the orbits,
followed by locating a lesion to its orbital compartment and clinical information will lead to the differential diagnosis.
However,
some lesions extend beyond these compartmental borders and effect more than one and up to all orbital compartments – again important to notice for the differntial diagnosis.
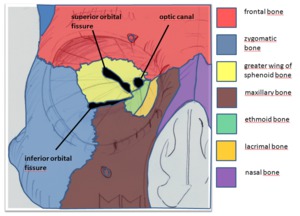
Fig. 2: Bony orbital anatomy.
The four orbital compartments:
- Ocular = ocular globe,
deliniated by sclera
- Orbital muscle and surrounding fascia form a cone-like intraorbital structure separating the intraconal from the extraconal compartment
- Orbital musculature and surrounding fascia (Zinn’s fascia) form the cone itsself referred to as conal compartment
In our pictorial review we define the orbital periphery as any orbital structure outside the orbital cone.
For didactic reasons and reasons of image analysis the orbital periphery can again be subdivided into three compartments: the extraconal intraorbital compartment (yellow),
the periosteal or subperistoeal compartment and the osseous compartment (=bony orbits,
coded in red).
Anatomic structures that are part of orbital anatomy are extraconal fat,
vessels (the most anterior segments of ophthalmic artery and vein),
lymphatics,
nerves (e.g.
V1 und V2 of trigeminal nerve),
lacrimal gland,
perosteum and the bony orbital structures including adjacent sinuses.
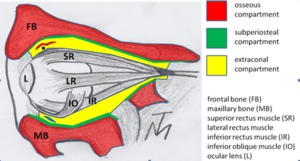
Fig. 5: Peripheral orbital anatomy.
Periorbital septum: The intraorbital space is bounded anteriorly by the periorbital septum.
Its is important to discern the periorbital or orbital septum,
in order to differentiate intraorbital from periorbital processes.
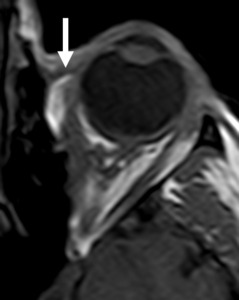
Fig. 6: Periorbital septum on axial T1W MR image.
Imaging of the orbital periphery heavily depends on CT or MRI and often both.
Ultrasound plays a minor role and is generally performed by ophthalmologists.
The osseous orbits are best visualized in CT,
however MRI and CT are performed complementary due the excellent soft-tissue contrast and functional capabilities of MRI and the depiction of bony structures in CT.


