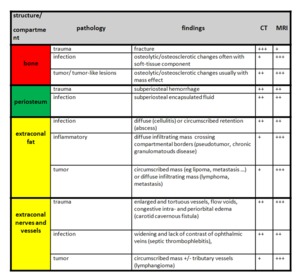
Fig. 7: Imaging findings of different orbital pathologies in their respective peripheral orbital compartment.
The following cases of our pictorial review show various pathologies affecting the extraconal space that we have recently seen in our day-to-day routine.
We have chosen to present them point by point covering:
1) trauma
2) infection
3) tumor and tumor-like lesions
In addition we will deal with pathologies originating from neighbouring structures that can affect the orbits.
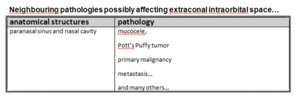
Fig. 8: Neighbouring pathologies possibly affecting the orbits.
Trauma
CT is the mainstay for evaluation of orbital trauma.
Orbital fractures can be isolated or be part of more complex facial fractures.
Bony fractures are evident as discontinuities of orbital osseous structures.
|
Isolated orbital wall fractures
|
Blow-in,
blow-out mechanism (fracture can also occur as part of a more complex fracture)
|
|
Nasoorbitoethmoid complex fractures (NOE)
|
fracture of frontal sinus,
ethmoid sinus,
anterior cranial fossa,
orbits,
frontal bone,
nasal bones
|
|
Zygomaticomaxillary complex fractures (ZMC)
|
tripod or malar fracture: fracture of maxillary sinus,
zygomatic arch,
lateral orbital rim or orbitozygomatic suture
|
|
Le Fort fractures
|
only Le Fort II and II involve orbits
|
|
Anterior skull base fracture
|
intracranial fracture,
usually involves orbital roof
|
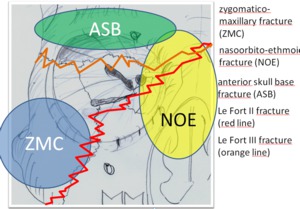
Fig. 9: Complex fractures involving the orbits.
CT and MRI are both useful in evaluating for incarcerated intraorbital content such as fat or muscles.
Special attention should be paid to optic nerve injuries which are beyond the scope of this article.
A possible sequela of orbital trauma is carotid-cavernous fistula which can occur within weeks after trauma.
Imaging findings include engorged and tortuous veins,
intra- and periorbital edematous changes.
Case: A 53 year-old patient with blow- out fracture on the left after trauma. There are concomitant hemorrhagic changes and herniation of intraorbital fat into the maxillary sinus.

Fig. 10: Blow out fracture left eye.
Case: A 17 year-old male after trauma of the right orbit.
Air outlining the ossesous orbits in the extraconal space as an indirect sign of fracture of the lamina papyracea.
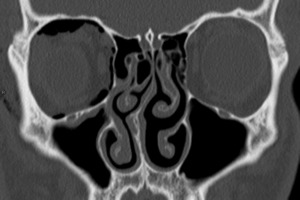
Fig. 11: Fracture of lamina papyracea.
Case: CT in a 43 presenting with bilateral orbital fractures.
Left –sided orbital roof fracture and fracture along the infraorbital canal (coronal CT image).
Orbital fracture on the right not displayed.
The patient presented 6 weeks afterwards with carotid-cavernous fistula on the right side.
MR images show engorged and tortuous right cavernous sinus and superior ophthalmic vein (arrows).

Fig. 12: Carotid-cavernous fistula.
Case: 20 year-old patient with severe head trauma due to motor vehicle accident presenting complex cranial and facial fractures involving the orbits on both sides.
There is fracture of the anterior skull base (arrows indicating fracture line and intracranial air) and Le Fort fracture lines II (red line) and III (orange line) can be seen.
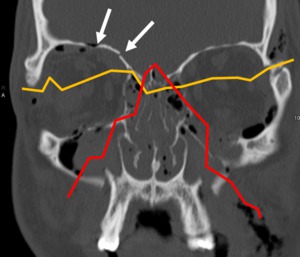
Fig. 13: Complex fracture.
Case: 22 year-old patient presenting with lateral orbital wall fracture (not shown) on the left as part of a more complex fracture.
Fracture of maxillary sinus and zygomatic arch (arrows) constitute tripod or zygomatico-maxillary complex fracture.
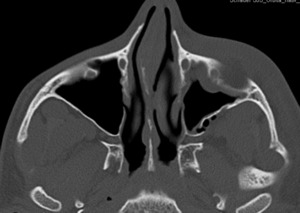
Fig. 14: Tripod fracture left-sided.
Infection
Infectious processes of the orbits can manifest as abscess or cellulitis.
It is important to diagnosis abscess formation aggressively.
Any circumscribed intraorbital opacity in CT in patients with suspected intraorbital infection should be diagnosed as intraorbital abscess.
Peripheral enhancement as required for abscess diagnosis in other areas is not required,
hence the diagnosis of an intraorbital abscess can be made even from an unenhanced CT scan.
Intraorbital cellulitis in CT is less circumscribed and a more diffuse intraorbital opacity compared to an abscess also without contrast enhancement.
However,
in children even delicate intraorbital opacities should be diagnosed as abscesses because the periorbital bony structures are a lot more fenestrated and disease spread occurs easily.
In cellulitis it is crucial to locate to process exactly with regard to the orbital septum,
since periorbital cellulitis can be managed on an outpatient base and orbital cellulitis generally requires hospital admission.
Complications of intraorbital infection include septic thrombophlebitis of inferior and superior ophthalmic vein.
Case: 45 year-old patient presenting to the ER with a red hot eye.
CT shows encapsulated lesion with peripheral enhancement in keeping with intraorbital abscess formation.
Coronal reformations reveal that the lesion is originating from the nasolacrimal duct.
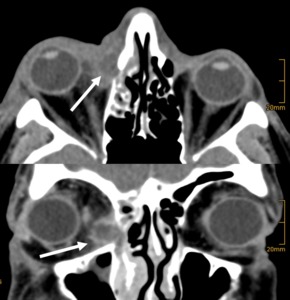
Fig. 15: Subperiosteal abscess.
Case: 28 year-old female presenting with a red hot eye on the left.
CT clearly shows opacities anterior to the periorbital septum (arrow),
so in this patient there is no intraorbital pathology.
The patient was successfully treated with antibiotics in an outpatient setting.
Symptoms gradually decreased over a period of 10 days and eventually resolved entirely.

Fig. 16: Periorbital cellulitis.
Tumor and tumor-like lesions
The list of orbital and periorbital tumors and tumor-like lesions is long and in most cases never complete.
We provide cases of orbital periphery tumors that we have recently seen.
The differential diagnosis is based on the orbital compartment that the lesion is originating from.
Furthermore morphologic criteria on T1W,
T2W,
fat suppressed images and after contrast administration are most important.
Recently,
diffusion weighted imaging has gained importance.
Low Signal intensity in T2W images is a typical finding for intraorbital lymphoma.
Some tumors are very rare and the likelyhood to make this diagnosis is low.
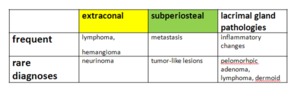
Fig. 17: Tumor encounted in the orbital periphery.
Case: 58 year-old female with diplopia and exopthalmus on the right,
MRI revealed a 5 cm large mass lesion originating from the extraconal space with areas showing loss of signal on fat suppressed images.
CT shows negative HU densities.
The lesion is a lipoma well demonstrating that fat is the radiologist’s friend.
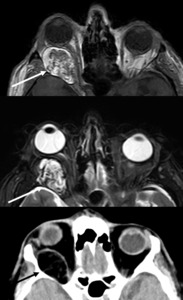
Fig. 18: Lipoma.
Case: Orbital MRI in a 69 year-old patient with extraconal mass displaying low SI on T1W an intermediate SI on STIR images.
The lesions shows nodular enhancement typical for hemangioma,
which is one of the most frequent orbital masses.

Fig. 19: Hemangioma.
Case: 70 year-old male patient with medial orbital wall fracture mor than 20 years ago and now presenting with a 1,5 cm large extraconal intraorbital mass showing low SI on T1W and high SI on T2W lesion,
there is no contrast enhancement.
Diagnosis is orbital mucocele a common finding after remote trauma.
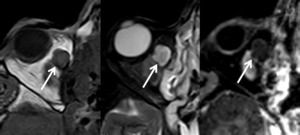
Fig. 20: Mucocele.
Case: 64 year-old female presenting with diplopia.
MRI shows bilateral orbital mass lesions predominantly in the extraconal space (arrows).
On the right the lesion extends into to intraconal space and displaces the optic nerve.
Histologic diagnosis was lymphoma.
Typical imaging findings included low SI on T2W images.
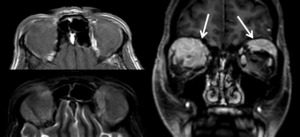
Fig. 21: Bilateral lymphoma.
Case: 43 year-old male presenting with visual loss on the left.
MRI shows a mass lesion at the tip of the orbital cone surrounding and compressing the optic nerve with avid contrast enhancement.
Differential diagnosis included lymphoma,
granulomatous disease or pseudotumor.
Histologic analysis yielded diagnosis of lymphoma
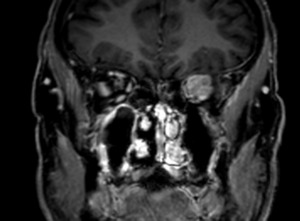
Fig. 22: Lymphoma at tip of left orbit.
Case: 20 year-old female presenting bony changes of maxillary,
ethmoid and sphenoid bones pathognonomic for fibrous dysplasia.

Fig. 23: Fibrous dysplasia
Case: 70 year-old female presenting osteoplastic lesion of the right frontal bone,
the bony orbit and the temporal bone.
The lesion displays low SI on T2,
there is thickening of the adjacent meninges.
Findings suggest intraosseous meningioma which was confirmed histologically.
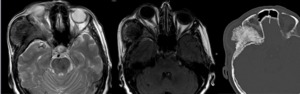
Fig. 24: Intraosseous meningioma.
Case: 57 year-old patient with osseous lesion of the frontal sinus and invasion of the right orbit.
There is a second lesion in the sphenoid wing on the right – both lesions were thought to be metastasis but histologic diagnosis was multiple myeloma.
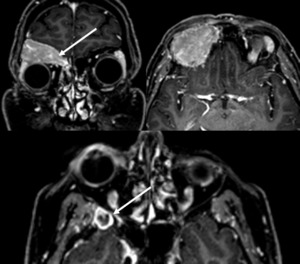
Fig. 25: Multiple myeloma.






