The first step in analyzing a pelvic tumor is to determine if it is intra or extra-peritoneal.
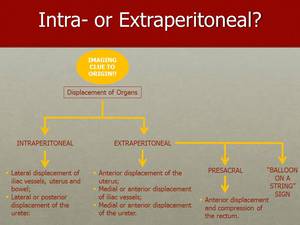
Fig. 5
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
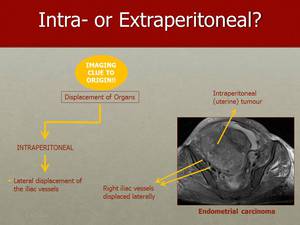
Fig. 6: If the tumour is intraperitoneal, the iliac vessels are displaced laterally by it, as it can be seen on this image of an endometrial carcinoma.
It helps to look at the contralateral side for comparison.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
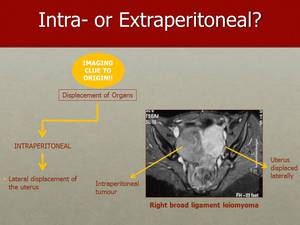
Fig. 7: This is a case of a leiomyoma of the right broad ligament, pushing the uterus laterally to the left.
The tumour is pushing the uterus laterally to the left, which allows us to localize it into the peritoneal space.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
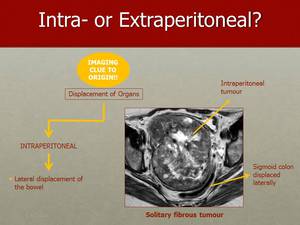
Fig. 8: An helpful sign of an intraperitoneal location of the tumour is the lateral displacement of the sigmoid colon, as observed in this example of a retro-vesical solitary fibrous tumour.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
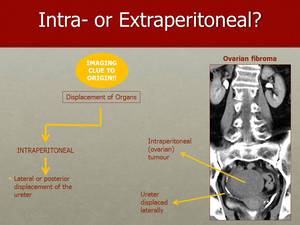
Fig. 9: To recognize that the tumour displaces the ureter laterally allow us to know that the tumour has an intraperitoneal origin, as in this case of right ovarian fibroma, pushing the ureter to the right.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
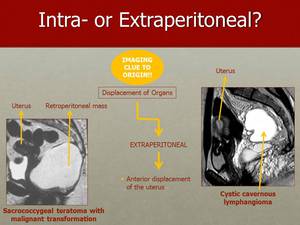
Fig. 10: Anterior displacement of the uterus is a sign of the extraperitoneal origin of the tumour.
On the left hand side you can see how this sacrococcygeal teratoma pushes the uterus anteriorly on the sagittal plane.
On the right hand side you can observe a cystic cavernous lymphangioma, pushing the uterus anteriorly.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
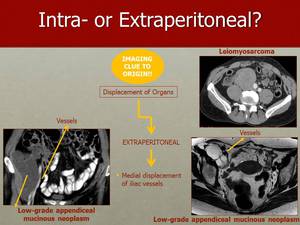
Fig. 11: In contrast with intraperitoneal masses, tumours with extraperitoneal origin cause medial displacement of the retroperitoneal vessels. Here you can observe medial displacement of the vessels pushed by a retroperitoneal leiomyosarcoma on CT and by a low-grade appendiceal mucinous neoplasm on CT and on axial T2WI.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
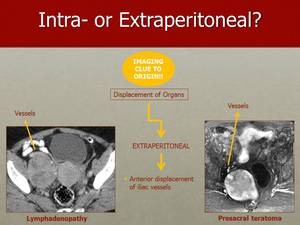
Fig. 12: The iliac vessels can also be pushed anteriorly by extraperitoneal tumours, as in these cases of an adenopathic conglomerate on the left hand side image and by a presacral teratoma on the right hand side image.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
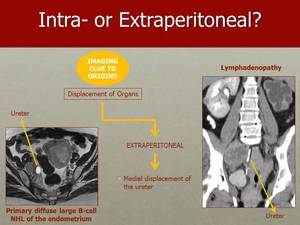
Fig. 13: In contrast with intraperitoneal tumous, extraperitoneal lesions cause medial displacement of the ureter, such as in these cases. On the left hand side there is medial displacement of the ureter due to enlarged internal iliac lymphadenopathy, from a primary diffuse large B-cell NHL of the endometrium. On the right hand side the right ureter is opacified and the medial displacement was caused by bulky confluent adenopathy.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
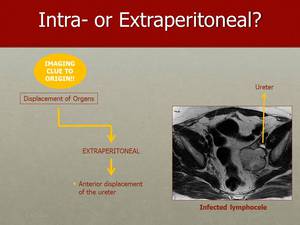
Fig. 14: As it happens to the illiac vessels, the ureter can also be pushed anteriorly by extraperitoneal tumours, as in this case of an infected lymphocele.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
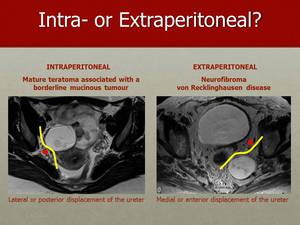
Fig. 15: On this slide we can appreciate the differences in displacement of the ureter, whether the tumor is intra or extra-peritoneal. The image on the left hand side shows a mature teratoma associated with a borderline mucinous tumor pushing the ureter laterally and posteriorly, indicating an intraperitoneal origin of the mass. The image on the right hand side shows a neurofibroma pushing the ureter medially and anteriorly, suggesting its extraperitoneal origin.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
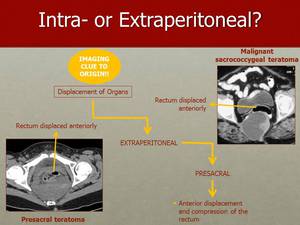
Fig. 16: Presacral tumours displace the rectum anteriorly, as one can observe in these cases of presacral teratomas.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
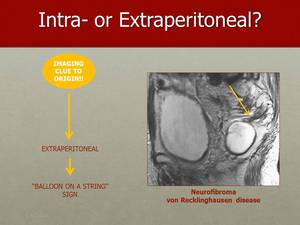
Fig. 17: The specific case of a neurofibroma can usually be suspected when the characteristic “Balloon on a String” sign is present.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
Moving on to the important distinction between ovarian or non-ovarian tumors,
there are a number of signs that can point us in the right direction.
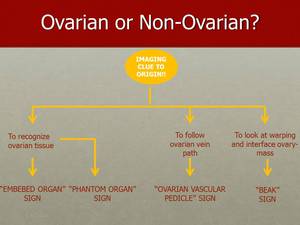
Fig. 18
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
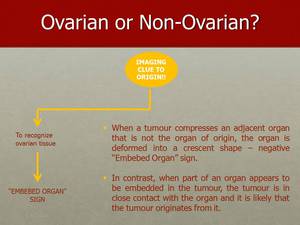
Fig. 19: The "Embedded Organ" sign indicates that the tumour originates from the ovary, due to loss of a separating plane of tissue, and absence of deformation of the organ due to extrinsic compression by the tumour.
It is important to be able to recognize at least some normal ovarian tissue, otherwise this sign will not be detectable. In many large tumours this is not possible.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
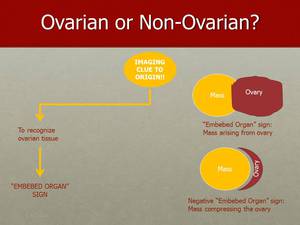
Fig. 20: In these two figures we can visualize what we look for when trying to determine if the "Embedded Organ" sign is present.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
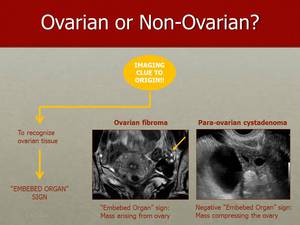
Fig. 21: Loss of a separating plane of tissue and absence of deformation of the organ due to extrinsic compression by the tumour – "Embedded Organ" sign – indicates that the tumour originates from the ovary, as in this cases of an ovarian fibroma clearly embedded within normal ovarian tissue (on the left hand side).
In contrast a para-ovarian cystadenoma compresses and deforms the ovary into a crescent shape but is not arising from the ovarian tissue itself – negative "Embedded Organ" sign (on the right hand side).
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
Fig. 22: The "Phantom Organ" sign is useful when you are not able to detect the organ of origin – which precludes the detection of the embedded organ sign.
A large tumour can make a small organ become undetectable, such as in the case of the ovaries.
The inability to detect the ovary itself, providing there is no history of surgical resection or transposition, is a clue that it is probably the organ of origin, and other anatomical landmarks can be of help.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
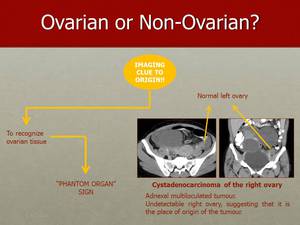
Fig. 23: In this case of a cystadenoma of the right ovary, the ovary itself became undetectable. The left ovary has a normal appearance, which should raise the suspicion of a right ovarian origin of this tumour.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
Fig. 24: Another clue that may be of help when determining either the origin of the tumour, or the side of an already established ovarian tumour, is the "Vascular Pedicle" sign.
The "Vascular Pedicle" sign is the presence of an enlarged gonadal vein in relation to the contralateral gonadal vein.
The distended vein indicates increased blood flow from a tumour on the ipsilateral side.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
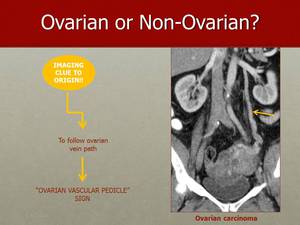
Fig. 25: In this image, the distended left gonadal vein, draining into the left renal vein, indicates increased blood flow from the tumour on the ipsilateral side, pointing out the origin of the tumour to the right ovary.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
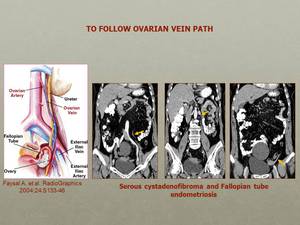
Fig. 26: Following the left gonadal vein from the left renal vein to the pelvis, on the ventral aspect of the ipsilateral iliopsoas muscle, will lead us to the suspensory ligament and the ovary.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
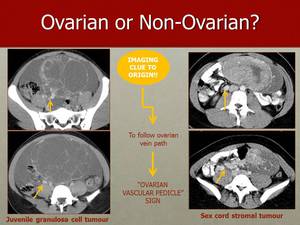
Fig. 27: In this image, we can see a large juvenile granulosa cell tumour (on the left) and a large sex cord stromal tumour (on the right), both of which produced a dilated ipsilateral gonadal vein (arrows), pointing to their origin through the "Vascular Pedicle" sign.
Is is of utmost importance to have relevant clinical history and examination data in relation to these patients – the presence of pain should raise the possibility of ovarian torsion, which can usually be detected by ultrasound.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
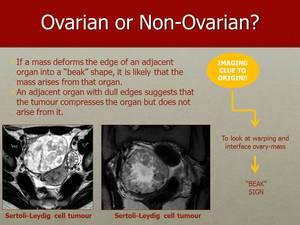
Fig. 28: The “Beak” sign is seen when the tumour arises from the ovary and makes the edges of normal parenchyma extend and wrap around the tumour.
Therefore there will be sharp angles between the ovarian parenchyma and the tumour as in these two cases of Sertoli-Leydig tumours.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
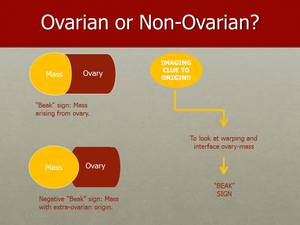
Fig. 29: The “Beak” sign consists of sharp angles between ovary and the lesion, which you can appreciate in these illustrations.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
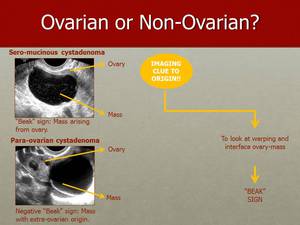
Fig. 30: The “Beak” sign is present on an ultrasound image of a sero-mucinous cystadenoma (on the top image). Absence of the “Beak” sign on an ultrasound image of a para-ovarian cystadenoma (on the bottom image).
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
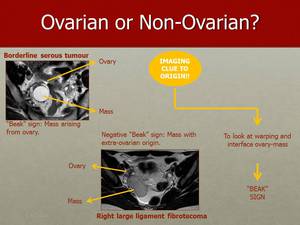
Fig. 31: The “Beak” sign produced by a borderline serous tumour of the right ovary (on the top image) and the absence of a “Beak” sign in a case of right broad ligament fibrotecoma (on the bottom image).
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
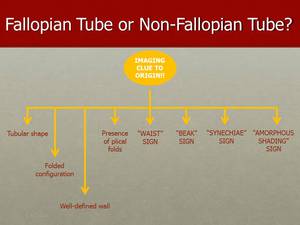
Fig. 32: When localizing pelvic tumours, it is very important to determine if the Fallopian tube is involved.
When the Fallopian tubes are visible, they usually have a tubular shape with a well defined wall and folded configuration.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
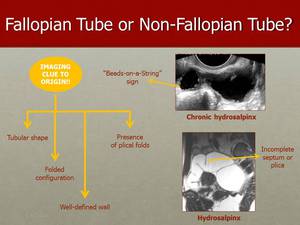
Fig. 33: The presence of a tubular and fluid filled structure (on the top image), that can be tortuous or serpentine is typical of an hydrosalpinx. The thin wall and small round projections, the "Beads-on-a-String" sign, are indicators of chronic disease. The presence of incomplete septa or plical folds, as we can see on the bottom image, are indicative of an hydrosalpinx.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
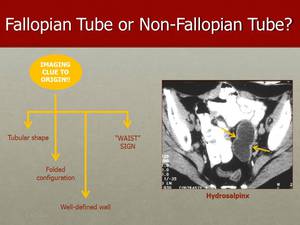
Fig. 34: On CT, hydrosalpinx in seen as a fluid-attenuation tubular structure with well defined walls, and with diametrically opposed indentations in the wall, which is the description of the "Waist" sign.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
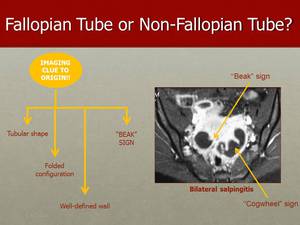
Fig. 35: In this image, we can see bilateral cystic tubular adnexal mass with a thick wall and incomplete septa - "Cogwheel" sign. The ‘‘Cogwheel” sign is an indicator of acute disease. The ‘‘Beak’’ sign is an acute angular contour feature. The presence of thickening and contrast-enhancement of tubal walls in association with inflammatory signs of adjacent structures, as densification of adnexal fat planes, are signs of salpingitis, as we can see in this case of bilateral salpingitis.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
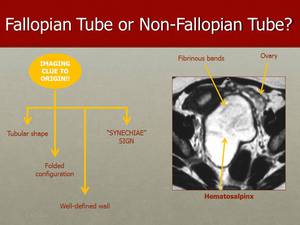
Fig. 36: The presence of an adnexal tubular structure, separated from the ovary, with synechiae, that are fine strands running across the lumen - "Synechiae" sign - is suggestive of tubal origin of the lesion, as we can see in this case of hematosalpinx, in which the luminal content presents high attenuating on CT and high signal on T2 MRI images, from altered blood products.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
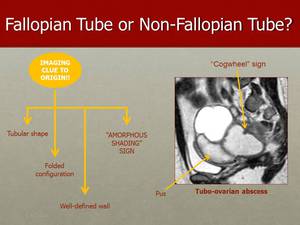
Fig. 37: This is another case of a Fallopian Tube lesion where is present the ‘‘Cogwheel’’ sign. The associated "Amorphous Shading" sign, that consists on amorphous signal loss or geographic shading (signal loss on T2W images), is suggesting of pus, such as in this case of tubo-ovarian abscess. It is different from the shading seen with the presence of blood products, such as in endometriosis, because there is no evidence of sedimentation or gravitational effects.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
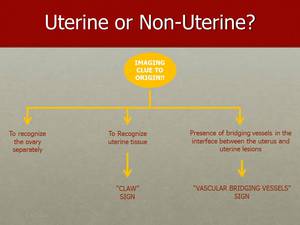
Fig. 38: A common pitfall includes misinterpretation of uterine leiomyomas as adnexal masses. So initially, adnexal "versus" non-adnexal has to be distinguished.
In subserous uterine leiomyomas tortuous vessels at the interface between uterus and the lesion – the "Bridging Vessel" sign helps identify extraovarian (uterine) origin.
Subserous leiomyomas may also display the "Claw" sign. Contrary to "Claw" sign there is a similar sign for lesions originating from the ovary. This is termed "Beak" sign and consists of sharp angles between ovary and the lesion.
Presence of follicles serves as another confident sign for ovarian origin.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
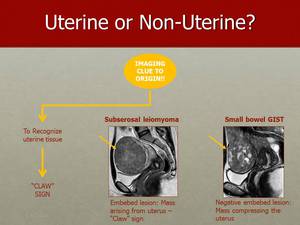
Fig. 39: A claw like extension of the myometrium surrounding the lesion is typically produced by subserosal uterine leiomyomas, such as the one seen on the left hand side MR image.
A negative "Claw" sign is seen in this case of small bowel GIST compressing but extrinsic to the uterus (on the right hand side).
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT
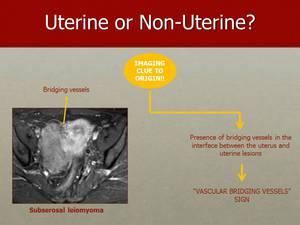
Fig. 40: The "Vascular Bridging Vessels" sign consists of the presence of bridging vessels in the interface between a subserosal leiomyoma and the uterus, as seen in this case.
References: Department of Radiology, Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon/PT

