In this section,
the commonest types of lymphoma will be discussed in further detail accompanied by relevant images.
Hodgkin’s lymphoma (HL) is characterised by the presence of Reed-Sternberg cells and their variants accompanied by an inflammatory background composed mainly of lymphocytes,
eosinophils and fibroblasts.
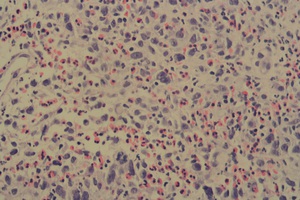
Fig. 1: High Power - Hodgkin's Lymphoma
Several large neoplastic lymphoid cells admixed with abundant eosinophils. Neoplastic cells are hyperchromatic with prominent nucleoli. Nodular sclerosing subtype, Hodgkin’s lymphoma.
References: Department of Pathology, Mater Dei Hospital, Msida, Malta
Mediastinal lymphadenopathy is the commonest presentation of HL with anterior and middle mediastinal lymph node involvement followed by retroperitoneal nodes [1].
Occasionally,
hilar lymphadenopathy may be present accompanied by lung involvement.
However,
studies show that the lungs are never involved in the absence of mediastinal disease[2].
Fig. 2: 19 year old lady presenting with right shoulder pain and B symptoms. CT and FDG-PET/CT were performed showing extensive right infraclavicular, paratracheal and subpectoral regions, anterior mediastinum, parasternal, right tracheobronchial, subcarinal and hilar lymphadenopathy with involvement of the right chest wall. No lung involvement is evident. Possible spleen involvement.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Fig. 3: PET-CT confirms increased FDG avidity in the regions described in Figure 2.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Extranodal manifestations of disease are also possible with liver and spleen being the commonest sites.
The main differential diagnoses of HL include mostly infectious diseases such as Cytomegalovirus,
Infectious Mononucleosis,
Syphilis,
Toxoplasmosis and Tuberculosis.
Sarcoidosis,
primary lung malignancies and autoimmune conditions may also have similar presentations.
Diffuse large B cell lymphoma (DLBCL) includes a heterogeneous group of neoplasms that exhibit diffuse proliferation of abnormal large B lymphocytes.
It represents more than 25% of all non-Hodgkin Lymphomas (NHL)[1].
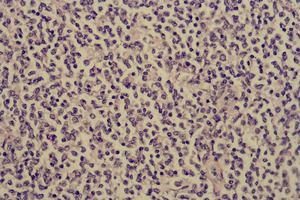
Fig. 4: High power - Lymph node
The lymph node parenchyma is almost completely effaced by a diffuse proliferation of neoplastic lymphocytes that have large nuclei with occasional prominent nucleoli.
References: Pathology Department, Mater Dei Hospital, Msida, Malta
Typical disease presentation involves a rapidly enlarging mass or masses that produce symptoms,
usually in the neck or abdomen.
More than half of the patients will present with advanced stage disease[3].
Primary DLBCL may present in the following tissues: gastrointestinal tract,
skin,
bone,
testis,
lung,
thyroid,
central nervous system,
breast and many others.
The differential diagnosis is vast and depends on original symptomatology; however,
infectious mononucleosis,
carcinoma,
melanoma,
sarcoidosis and other types of lymphoma should always be considered.
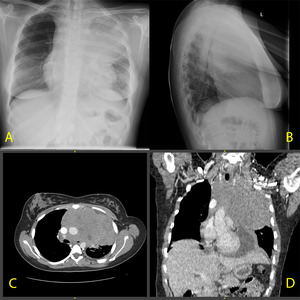
Fig. 5: A. CXR PA and Lateral (A,B) . CT axial (C). CT coronal reconstruction (D)
An 18 year old girl who presented with B symptoms.
The CXR shows a large mediastinal mass. A CT of the neck and trunk was performed that exhibited a large, relatively homogeneous mass in the anterior and middle mediastinum which encased the vessels and was compressing both pulmonary arteries and the left main bronchus. The mass was reaching proximally and protruded into the thoracic inlet. There were enlarged lymph nodes in the supraclavicular, parasternal and prepericardial groups. A moderate pericardial effusion is also demonstrated.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
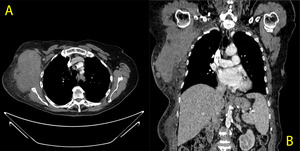
Fig. 6: A. CT axial B. CT coronal reconstruction
82 year old lady who presented with a large firm mass over her right shoulder with overlying bruising.
The images show a large solid moderately vascularised mass with a maximal size of 13 cm in the right axillary fossa. Multiple enlarged lymph nodes and collateral vessels are present.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Extranodal disease is present in 40% of patients with DLBCL [4].
Primary non-Hodgkin lymphoma of the gastrointestinal tract (GIT) is rare and accounts for a very small number of primary GIT malignancies [5,6].
However,
the gastrointestinal tract is the commonest site of secondary involvement by lymphoma [6,7].
The most common histological presentations include extranodal marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALT),
DLBCL,
mantle cell lymphoma and occasionally T-cell neoplasms.
The stomach (up to 75 %) and the small bowel (most commonly the ileum) are the commonest sites [6] of involvement.

Fig. 7: A. CT axial B. CT coronal
58 year old gentleman who presented with melaena. A friable mass was seen by endoscopy on the junction of the 2nd and 3rd part of the duodenum. On CT, asymmetrical mural thickening (up to 35mm) of the duodenum is seen along with a mildly enlarged regional lymph node. Histology showed DLBCL of the duodenum.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Lymphoma of the testis is an uncommon type of extranodal non-Hodgkin lymphoma.
It tends to present in patients who are more than 60 years of age and accounts for about 9% of all testicular neoplasms.
It has been described as the commonest testicular malignancy in elderly men.
Bilateral testicular involvement is present in 16-36% of patients [8,9].
Patients tend to present with a testicular mass and occasionally with B symptoms.
CNS involvement is possible.
Many other primary testicular tumours may have a similar presentation.
Germ cell tumours such as seminoma and teratoma account for the vast majority of neoplasms. Testicular sex-cord stromal tumours and mixed neoplasms should also be included in the differential diagnosis.
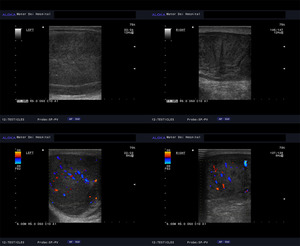
Fig. 8: 56 year old gentleman with a rapidly growing left, hard and irregular testicular mass. Both testicles exhibit an abnormally heterogeneous echotexture with increased Doppler flow and bilateral hydrocoeles. Histology confirmed primary diffuse large B cell lymphoma. Though unlikely in this particular case, metastatic disease should be considered as a differential diagnosis.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Follicular lymphoma is the second commonest lymphoma in the Western world [1].
The neoplastic cells are derived from germinal centre B cells that exhibit a follicular growth pattern.
Transformation to high grade lymphoma may occur in up to 70% of patients over time [1,10-11]. Presentation usually consists of peripheral,
painless,
often massive lymphadenopathy and B symptoms.
The cervical,
axillary and inguinal lymph node groups are most commonly involved.
Occasionally,
presentation may include a large abdominal mass that causes obstructive gastrointestinal and urinary symptoms.
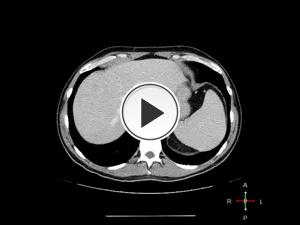
Fig. 9: CT axial. 44 year old gentleman who presented with left inguinal lymphadenopathy and lethargy. On CT, there is diffuse retroperitoneal and abdominal lymphadenopathy extending to the level of the urinary bladder. There is Grade I hydronephrosis of the left kidney secondary to compression from the enlarged lymph node group. Typically, retroperitoneal lymphoma/malignancy displaces ureters laterally and aorta anteriorly. Less aortic displacement and medial displacement of ureters (so-called "maiden waist" deformity of ureters on CT IVU) is characteristic of Retroperitoneal Fibrosis.
References: Medical Imaging Department, Mater Dei Hospital, Malta
Patients with follicular lymphoma tend to have disseminated disease on presentation.
One staging series concludes that the spleen is involved in 40% of cases,
the liver in 50% and bone marrow in up to 80% of cases[11].
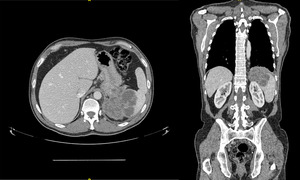
Fig. 10: A. CT axial B. CT coronal
58 year old gentleman presenting with lethargy and B symptoms.
The CT shows a large lobulated and septated mass in the spleen measuring approximately 9 cm. There are also enlarged retroperitoneal lymph nodes at the level of the kidneys and the internal iliac group.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Marginal zone B cell lymphoma (MZL) usually arises from post-germinal centre marginal zone B cells surrounding normal lymphoid follicles.
There are three subclassifications of MZL that share the same immunophenotype: MALT lymphoma,
Splenic MZL and Nodal MZL.
Marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT) tends to involve the gastrointestinal tract (most commonly the stomach and small bowel),
lung,
salivary gland,
orbital adnexa and thyroid gland.
Presenting features vary greatly according to the tissue that is involved.
Disseminated disease,
involving lymph nodes or bone marrow has been reported in up to one third of patients[12].
Pulmonary marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT) is relatively rare compared to gastrointestinal MALT lymphoma.
In one series,
approximately 40% of patients were found to be asymptomatic at the time of diagnosis.
62% of patients had only single lobe involvement in comparison to 25% of patients with bilateral involvement[13].
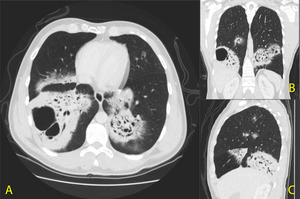
Fig. 11: A. CT axial B. CT coronal C. CT sagittal - 45 year old gentleman with a 6 month history of persistent cough productive of yellowish sputum. On the first CT examination, multiple areas of patchy consolidation are seen bilaterally with cavitation and no visible fluid level. No pattern of distribution is evident, however, the lower lobes are mostly affected.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta
Marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT) is also known to affect the ocular adnexa and is in fact,
the commonest primary orbital neoplasm in the elderly population [14,15].
Patients generally present with proptosis,
diplopia and restricted eye movements ( Fig. 12 ).
The ability to differentiate malignant lymphoma from benign conditions or other tumours is not well established.
A significant feature of lymphoma within the orbit is its tendency to ‘mold’ to orbital structures[14].
The differential diagnosis should include rare benign diseases such as cavernous malformations and hemangiopericytoma,
tumours of the nervous tissue such as optic nerve glioma and schwannomas and finally,
melanoma which is the most common intraocular malignancy in adults[14].
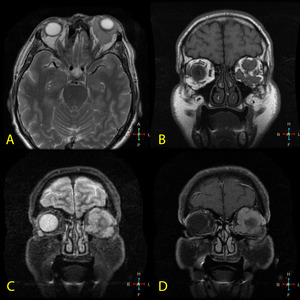
Fig. 13: A. MR axial T2 weighted B. MR Coronal T1 weighted FE C. MR Coronal STIR D. MR Coronal T1 + contrast.
61 year old gentleman with gradual proptosis and decrease in visual acuity. MR sequences show a left intraorbital (intra- and extra-conal) lobulated mass causing significant left proptosis. It engulfs the extra-conal muscles and lacrimal gland. Histology of the conjunctiva and mass confirmed involvement by lymphoma.
References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta



 . CT axial (C). CT coronal reconstruction (D)
An 18 year old girl who presented with B symptoms.
The CXR shows a large mediastinal mass. A CT of the neck and trunk was performed that exhibited a large, relatively homogeneous mass in the anterior and middle mediastinum which encased the vessels and was compressing both pulmonary arteries and the left main bronchus. The mass was reaching proximally and protruded into the thoracic inlet. There were enlarged lymph nodes in the supraclavicular, parasternal and prepericardial groups. A moderate pericardial effusion is also demonstrated. References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta")

 of the duodenum is seen along with a mildly enlarged regional lymph node. Histology showed DLBCL of the duodenum. References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta")




 lobulated mass causing significant left proptosis. It engulfs the extra-conal muscles and lacrimal gland. Histology of the conjunctiva and mass confirmed involvement by lymphoma. References: Medical Imaging Department, Mater Dei Hospital, Msida, Malta")