Percutaneous vertebroplasty (PVP) and balloon kyphoplasty (BKP) are vertebral augmentation techniques,
originally designed to treat painful vertebral collapse caused by aggressive hemangiomas.
Nowadays,
there are many other indications such as osteoporotic vertebral collapse,
osteolytic metastases,
multiple myeloma,
Langerhans cell histiocytosis and burst fractures.
Percutaneous vertebroplasty has been introduced by Galibert and Deramond in 1987,
and balloon kyphoplasty was executed for first time by Reiley et al.
in 1994.
More than 38,000 vertebroplasties and 16,000 kyphoplasties are performed yearly in the United States 1.
The aim of both techniques is to relieve pain,
to restore the vertebral height and to hinder the progression of kyphosis deformity.
They involve an injection of acrylic cement (polymethylmethacrylate [PMMA]) under fluoroscopic monitoring with a needle through the pedicles into the spongy bone of the collapsed vertebral body,
resulting in a partial remodelling of the vertebral body 2.
The injection of cement in PVP occurs without prior inflation of the diseased vertebrae,
ie.
under high pressure.
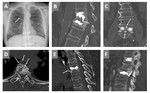
Balloon kyphoplasty (BKP) was introduced as a modification of vertebroplasty in which two inflatable balloons are introduced firstly through the transpedicular cannulas to create a cavity in the collapsed vertebral body.
This cavity allows the cement to be injected under lower pressure which minimizes extravasation (Fig.
1 & 2) 3.
The mechanism by which the injected cement provides pain relief is not fully understood.
The most accepted hypotheses are in the first place the thermal necrosis of the pain receptors in the vertebral body from a high temperature of the polymerisation of PMMA ( 122 C°) and secondly the mechanical effect of cement through the consolidation of microfractures with an additional role in pain relief.
The amount of injected cement varies according to the vertebral level: 3-6 ml is usually used in the lumbar vertebrae and 2-3 ml is used for the thoracic ones 4.
Literature concerning complications of percutaneous vertebroplasty and balloon kyphoplasty are gradually increasing,
mostly due to a widespread practice of these minimally invasive procedures because of their potential effectiveness in relieving pain.
Extravertebral cement leakage is the most frequently reported complication and occurs particularly when the needle tip is close to the fractured endplate.
This leakage of cement is either local into the disc,
spinal canal,
intervertebral space,
perivertebral venous system or a distant migration to the azygos vein,
inferior vena cava,
right heart and pulmonary circulation (Fig.
3) 5.
Fortunately most of reported cases with cement leakage are asymptomatic,
but pulmonary embolisms can be potentially fatal.
The patients with symptomatic cement embolisms are usually presented with dyspnea,
tachypnea,
chest pain,
coughing,
hemoptysis,
tachycardia,
cyanosis,
dizziness and sweating,
which makes it necessary to perform chest radiograph or CT.
Asymptomatic cement embolism is usually underestimated,
because there is no indication for chest radiological investigations.
The incidence of cement pulmonary embolism is variable in medical literature (30%-75% for vertebroplasty,
8.6%-33% for kyphoplasty) 6,7,8.
The aim of this retrospective study is to assess the incidence,
the characteristics and the risk factors of cement pulmonary embolism (CPE) after percutaneous balloon kyphoplasty in 68 patients with 162 treated vertebrae.
The authors compared the results with those from previous reports with reviewing the medical literature.

.")
.")