Before discussing rectal pathology and its imaging,
it is vital to be acquainted with the regional anatomy.
The rectum is the lowest part of the gastrointestinal tract.
Its histological structure similar to that of the colon with one important difference: whereas the colon is surrounded by an outer layer of connective tissue called the serosa,
meanwhile the rectum,
mostly is surrounded by fatty tissue,
the mesorectum.
The mesorectum contains lymph nodes,
vessels,
and several fibrous septa.
A thin layer of connective tissue,
the mesorectal fascia,
limits the mesorectum and separates it from the other structures in the pelvis (Figure 1).
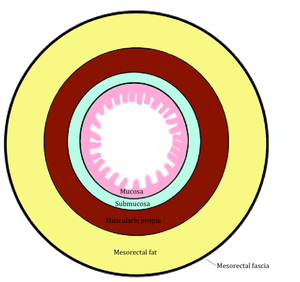
Fig. 1: Figure 1. Simplified scheme of histological layers of the rectum. NB: unlike colon, most of the rectum does not have serosa. In the TNM staging system of colon cancer, invasion of the serosa represents stage T3. However, in the case of rectal cancer T3 corresponds to the invasion of mesorectum.
References: Manuel Gutiérrez Gimeno. Department of Radiology, Hospital General de Catalunya, Barcelona, Spain.
The internal anal sphincter arises from the continuation of the inner circular part of the muscularis propria of the rectum.
The external anal sphincter is composed of three parts: a subcutaneous part,
a superficial part and a deep part.
The levator ani muscle is continuous with the external anal sphincter.
It loops around the anorectal junction,
and controls the anorectal angle,
being a key factor in faecal continence and defecation (Figure 2).
In developed countries,
rectal cancer, together with colon cancer,
is the third leading cancer in men after prostate and lung cancer,
and the second in women after breast cancer(1).
In the European Union,
the crude incidence of rectal cancer is 35% of the total colorectal cancer incidence (2).
Most colon and rectal cancers are adenocarcinomas (95-98%),
discussed in this poster; the remaining 2-5% include lymphomas,
sarcomas and carcinoid tumours (3).
The prognosis of rectal cancer after surgical treatment depends on several factors:
-
the histologic grade of the tumor
-
the extension of the tumoural tissue:
-
Limited to rectal wall (T1/T2)
-
Invasion of mesorrectal fat without invasion of the mesorrectal fascia (T3)
-
Invasion of mesorrectal fat with invasion of the mesorrectal fascia (T3)
-
vascular or perineural invasion (4)
-
the involvement of lymphatic nodes
Mesorectal fascia invasion is thought to be the most powerful predictor for local recurrence.
Mesorectal fascia is considered invaded when the distance between the deepest tumoural tissue and the fascia is 1mm or less.
In surgery,
this concept is regarded as the circumferential resection margin (CRM).
The CRM is considered positive when there are tumour deposits within 1 mm or less of the fascia,
and negative when the distance to the fascia is more than 1 mm.
Tumours with involvement of the mesorectal fascia (positive CRM) have a higher risk of recurrence than those without such involvement (negative CRM) (5–8).
The TNM staging system (9),
summarized in Table 1,
reflects the extension of the tumoural tissue within the rectal wall and the pelvis and indicates the involvement of lymphatic nodes.

Table 1: Table 1. AJCC guidelines for staging colon and rectal cancer.
References: Classification adapted from the American Joint Committee on Cancer staging system. Sub stages of T3 lesions are adapted from the RSNA Radiology Reporting Templates
The regional nodal group is composed of all perirectal lymph nodes and lymph nodes along the sigmoid arteries.
External iliac or common iliac nodes are not considered regional lymph nodes so their involvement represents M1 disease (4).
See Figure 3 for a simplified view of T stage in rectal cancer.
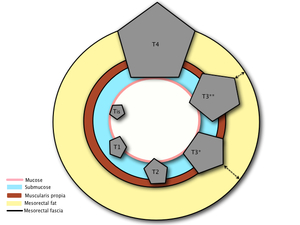
Fig. 3: Figure 3. T stages in rectal cancer. From left to right (counterclockwise): Tis (only mucosa is invaded). T1 (invasion of mucosa and submucosa), T2 (growing through the submucosa and extension into the muscularis propia), T3 (extension through the muscularis propia and invasion of mesorectal fat), T4 (direct invasion or adhesion to adjacent organs). In T3 stages the distance to mesorectal fascia is of major importance. T3 tumors with a CRM of 1mm or less are more likely to recur than tumors with a wide CRM.
References: Manuel Gutiérrez Gimeno. Department of Radiology, Hospital General de Catalunya, Barcelona, Spain.
After the recent multidisciplinary meeting of colorectal cancer (EURECCA) an imaging algorithm for rectal cancer (Figure 4) was suggested,
outlining the importance of correct staging of the local tumor extension,
with a special attention to:
-
contact with sphincter and the peritoneal reflection,
-
CRM margins and mesorectal fascia evaluation,
-
venous invasion.
(10)
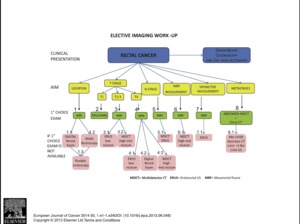
Fig. 4: Figure 4. Proposed imaging algorithm by EURECCA consensus document.
References: 2013 Elsevier Ltd. European Journal of Cancer 2014 50, 1.e1-1.e34DOI: (10.1016/j.ejca.2013.06.048)
The different techniques of rectal cancer imaging are discussed in the section of Findings and procedure details.



: Tis (only mucosa is invaded). T1 (invasion of mucosa and submucosa), T2 (growing through the submucosa and extension into the muscularis propia), T3 (extension through the muscularis propia and invasion of mesorectal fat), T4 (direct invasion or adhesion to adjacent organs). In T3 stages the distance to mesorectal fascia is of major importance. T3 tumors with a CRM of 1mm or less are more likely to recur than tumors with a wide CRM. References: Manuel Gutiérrez Gimeno. Department of Radiology, Hospital General de Catalunya, Barcelona, Spain.")

")