ECR 2015 / C-1980
Congenital absence of inferior vena cava
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1980
Type:
Educational Exhibit
Keywords:
Cardiovascular system, Veins / Vena cava, Abdomen, CT, MR, Ultrasound, Computer Applications-3D, Congenital, Dilatation, Dysplasias
Authors:
E. Kalchev, R. D. Popova, G. Valchev, B. Balev; Varna/BG
DOI:
10.1594/ecr2015/C-1980

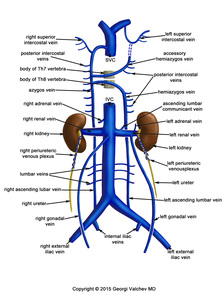
Fig. 1:
Normal blood drainage by the main venous vessels.
, portal vein (black arrow), splenic vein (black open arrow), superior mesenteric vein (white arrow). No flow in the inferior vena cava is seen. References: Department of Diagnostic Imaging, St. Marina University Hospital, Varna/ Bulgaria")
Fig. 2:
3D reconstruction of a CECT in the venous phase. Abdominal aorta (white open...
. References: Department of Diagnostic Imaging, St. Marina University Hospital, Varna/ Bulgaria. See references.")
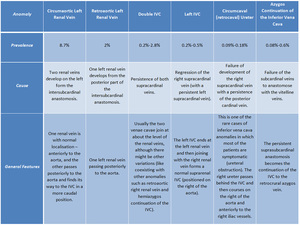
Table 1:
Anomalies of the inferior vena cava (besides absence of the IVC).
 in a patient with an absent inferior vena cava. References: Department of Diagnostic Imaging, St. Marina University Hospital, Varna/ Bulgaria")
Fig. 3:
MRI coronal image demonstrating dilated ascending lumbar veins (arrows) in a...
 ascending next to the thoracic aorta (white arrow). References: Department of Diagnostic Imaging, St. Marina University Hospital, Varna/ Bulgaria")
Fig. 4:
CT showing a dilated azygos vein (open arrow) ascending next to the thoracic...

Fig. 5:
CT demonstrating a dilated azygos vein draining into the superior vena cava.