Cerebral venous thrombosis (CVT),
Posterior reversible encephalopathy syndrome (PRES) and Reversible cerebral vasoconstriction syndrome (RCVS) may have similar clinical presentation,
being non-specific and usually variable,
what makes radiological exams play a crucial role (Fig.3).
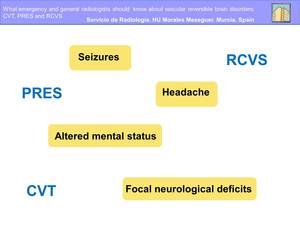
Fig. 3
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Posterior reversible encephalopathy syndrome (PRES):
It is a radiological and clinical entity characterised by a variety of symptoms including headache,
altered mental status,
seizures and visual disturbances,
and by a potentially reversible imaging pattern.
There are a number of factors that favour the development of this syndrome (Fig.4)
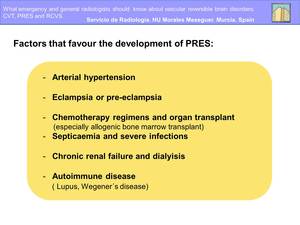
Fig. 4
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Although the pathophysiology remains unknown,
the currently preferred explanations relates to hypertension,
impaired autoregulation and hyperperfusion.
This theory suggests that severe hypertension exceeds the limits of autoregulation,
leading to breakthrough brain edema (Fig.5)
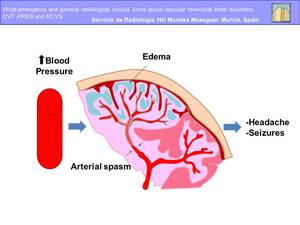
Fig. 5
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Clinical aspects
There are a range of neurological presentations that often involve generalised seizures,
sometimes complicated with status epilepticus in combination with headaches,
confusion,
nausea and vomiting.
There may be focal neurological deficits,
such as cortical blindness,
cerebral syndrome or hemiparesis.
This presentations may lead to coma (Fig.6) .
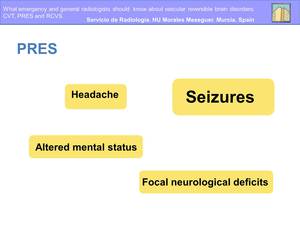
Fig. 6
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Typical imaging features:
On CT/MR imaging,
the brain typically demonstrates focal regions of symmetric hemispheric edema.
The parietal and occipital lobes are the most commonly affected,
followed by the frontal lobes,
the inferior temporal-occipital junction and the cerebellum.
On computed tomography,
diffuse hypodense areas indicate the affected regions.
On MRI,
lesions appear as isointense or low signal intensity on T1 weighted images,
and high signal intensity on T2 weighted images and FLAIR.
Enhancement is not usually seen after injection of a contrast agent.
On diffusion weighted imaging,
an increase in the diffusion coefficient can be seen,
connected to the presence of a vasogenic edema secondary to a dysfunction of the cerebrovascular autoregulation mechanisms.
Three primary variations of the traditional PRES imaging pattern are recognized (Fig.
7):
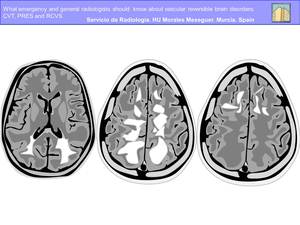
Fig. 7
References: Department of Radiology, Hospital General Universitario Morales Meseguer
-Primary Parietal-Occipital Pattern. The typical “posterior” pattern is present with involvement of the parietal and occipital cortex and white matter with variable involvement of the temporal lobes.
-Holohemispheric Watershed Pattern. Vasogenic edema is present in a linear pattern spanning the frontal,
parietal,
and occipital lobes,
with lesser involvement of the temporal lobes.
Reduced involvement of the cortex or deep white matter typically appears as non confluent cortical vasogenic edema,
which is most commonly identified along the superior frontal sulcus or a “string-of pearl” pattern of linearly arranged,
disconnected white matter edema .
-Superior Frontal Sulcus Pattern. The frontal abnormality tend to be linear and is located along the mid to posterior aspect of the superior frontal sulcus.
-Partial or Asymmetric Expression of the Primary Patterns.
It is the incomplete expression of these primary PRES patterns .The frontal lobes are frequently involved in these patients,
with either a linear pattern or a patchy,
disconnected linear arrangement.
Prognosis
In most patients,
imaging abnormalities are regressive after appropriate therapy,
suggesting transient edema rather than true infarction.
Follow-up studies may be key in the diagnosis because initial differentiation between a reversible and permanent parenchymal lesion .The ideal timing of repeated brain imaging to document recovery is unclear; resolution of PRES neuroimaging abnormalities probably occurs in the range of several days to weeks.
Cerebral Venous Thrombosis (CVT):
Cerebral venous thrombosis (CVT) is a rare type of cerebrovascular disease that can occur at any age,
including neonates.
The diagnosis is still commonly overlooked or delayed because of the remarkable diversity of its clinical symptoms,
modes of onset and neuroimaging signs.
Several disorders can cause or predispose patients to CVT.
These disorders may be classified as local (related to intrinsic or mechanical conditions of the cerebral veins and dural sinuses) or systemic (related to clinical conditions that promote thrombosis).
Local processes that alter the venous flow may potentiate the development of thrombosis (Fig.8).
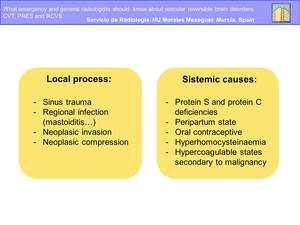
Fig. 8
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Recent studies have emphasized the role of hyperhomocysteinaemia.
This disorder is an independent and strong risk factor for CVT.
In as many as 25% of cases,
no cause is identified.
The pathophysiology of brain parenchymal involvement in venous occlusion differs from the arterial occlusion.
Parenchymal changes may be secondary to cytotoxic edema,
vasogenic edema,
or intracranial hemorrhage.
The primary mechanism is the increased venous pressure.
If collateral pathways of venous drainage are insufficient,
parenchymal changes may occur.
If venous pressure continues increasing,
with a consequent diminishment in arterial perfusion pressure,
cell death may ensue.
If adequate collateral pathways develop or recanalization occurs before cell death or intracranial hemorrhage,
the parenchymal changes may resolve partly or completely.
Clinical aspects:
The clinical manifestations of cerebral venous thrombosis vary depending on the extent,
location,
and acuity of the venous thrombotic process as well as the adequacy of venous collateral circulation.
The most common symptoms and signs are headache,
seizures,
focal neurological deficts,
altered consciousness and papilloedema,
wich can be presented isolated or in association with other symptoms (Fig.9).
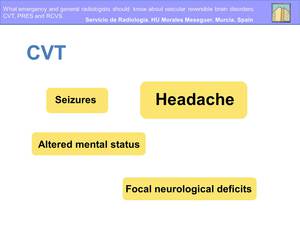
Fig. 9
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Headache is by far the most common initial symptom,
for this reason it is important to recognise CVT in patients with isolated headache in order to start treatment as early as possible.
Seizures are more typical in patients with parenchymal lesions,
sagittal sinus and cortical vein thrombosis,
and motor or sensory defects.
Patiens with chronic course or delayed clinical presentation may show papilloedema on fundoscopy; this finding is less common in acute cases.
When the deep cerebral venous system is occluded,
the clinical picture is usually more severe with coma,
mental troubles,
and motor deficits,
which are usually bilateral.
Typical imaging features:
The intracranial venous system may show a wide range of normal variations.
Magnetic resonance imaging (MRI) combined with magnetic resonance venography have replace invasive cerebral angiography and conventional computer tomography (CT).
And it allows the visualization of a greater number of venous structures (Fig.10).

Fig. 10: Scheme of Magnetic Resonance Venography.
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Although the venous drainage territories of the superficial cerebral brain are variable,
general drainage areas can be identified (Fig.11)
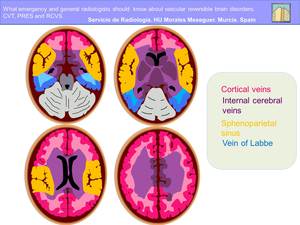
Fig. 11: Superficial cortical venous drainage territories
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Imaging findings:
Venous thrombi can be detected by direct visualization on MR and CT parenchymal images (Fig.
12).
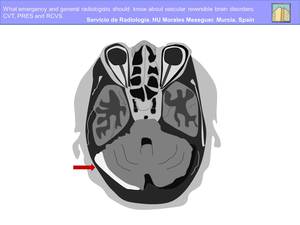
Fig. 12
References: Department of Radiology, Hospital General Universitario Morales Meseguer
The classic finding of sinus thrombosis on unenhanced CT images is a hyperattenuating thrombus in the occluded sinus.
However,
the increased attenuation in the venous sinuses is a relative uncommon findings and can also be seen in other causes like dehydration,
elevated haematocrit level,
or subjacent subarachnoid or subdural haemorrhages.
A well-known finding of sinus thrombosis on contrast-enhanced images is the empty delta sign,
a central intraluminal filling defect that represents the thrombus surrounded by contrast-enhanced dural collateral venous channels and cavernous spaces within the dural envelope.
Unenhanced MR imaging is more sensitive than unenhanced CT for the detection of venous thrombi.
The signal intensity of venous thrombi on T1- and T2-weighted MR images varies according to the interval between the onset of thrombus formation and the time of imaging.
The change in signal intensity is thought to be related to the paramagnetic effects of the products of hemoglobin breakdown in the thrombus (Fig.13).
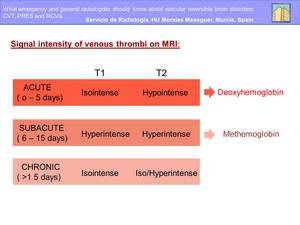
Fig. 13
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Gradient-recalled echo (GRE) sequences may be an important diagnostic aid in acute-stage thrombosis,
when the signal intensities on T1- and T2- weighted images may be more subtle.
Besides,
evolutioned thrombus in which paramagnetic products such as deoxyhemoglobin and methemoglobin are present,
the sensitivity of GRE sequences to magnetic susceptibility produces blooming artifacts in the thrombosed venous segments on GRE images.
There has been recent interest in evaluating the appearance of intraluminal venous thrombi on diffusion-weighted images.
Signal hyperintensity in thrombosed sinuses on diffusion weighted images,
with corresponding diminishment in the mean apparent diffusion coefficient (ADC) values,
has been described in 41% of patients with sinus thrombosis.
Prognosis:
Between 57-86% of patients have complete functional recovery.
Although there’s no clear correlation between disease severity and outcome,
several factors are associated with a poorer prognosis.
These are,
infancy and advanced age,
rapid onset with coma and focal deficits,
and thrombosis affecting the deep venous system.
The underlying conditions,
particularly sepsis and malignancy can adversely affect outcome
Reversible cerebral vasoconstriction syndrome (RCVS)
It is an under-recognized clinical-radiologic entity characterized by a history of sudden severe headaches,
sometimes associated with ischemic or hemorrhagic stroke,
focal neurologic deficits,
or seizures.
This condition is defined by reversible segmental cerebral vasoconstriction on angiography.
The angiographic findings are similar to those of other vasculopathies,
including PACNS (primary angiitis of the CNS).
Unlike PACNS,
the vascular abnormalities of RCVS resolve within several months.
Although the pathophysiology is not clearly understood,
a disturbance in the control of cerebral vascular tone seems to be a critical element.
This alteration in vascular tne may be spontaneous or evoked by exogenous or endogenous factors.
It typically occurs following exposure to a trigger,
commonly sympathomimetic or vasoactive agents.
Most patients with RCVS are young and middle-aged women ( Fig.14).
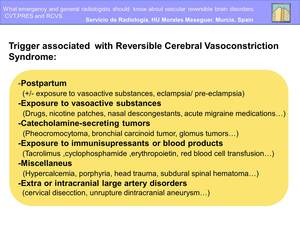
Fig. 14
References: Department of Radiology, Hospital General Universitario Morales Meseguer
Because management and outcome of RCVS differs from those of other vasculopathies,
it is critical that radiologists recognize its typical imaging appearance,
time course,
and clinical features.
Clinical aspects
Headache is the main symptom and often remains the only manifestation of RCVS.
It is typically bilateral,
although it can be unilateral.
Onset is acute with thunderclap headache,
extreme head pain peaking in less than 1minute,
mimicking that of a ruptured aneurysm (Fig.15)
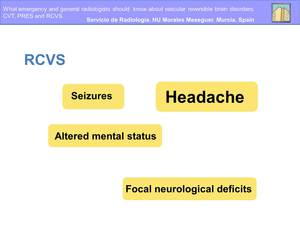
Fig. 15
References: Department of Radiology, Hospital General Universitario Morales Meseguer
In contrast with the headache associated with rupture aneurysms,
the severe pain of RCVS is short live (usually lasting 1- 3 h).
Thunderclap headaches usually are short (minutes) but cases lasting several days have been reported.
A single attack is possible,
but patients usually have a mean of four attacks during 1-4 weeks.
In some patients,
headache is more progressive and less severe than in typical cases,
but the absence of headache at onset is exceptional.
Focal deficits,
which can be transient or persistent,
and seizures have been reported in 8-43% and 1 -17% respectively.
Most focal deficits have a sudden onset and are similar of those noted in transient ischaemic attacks,
but they can mimic a migraine aura.
Persistent deficits,
including hemiplegia,
aphasia ,hemianopia or cortical blindness suggests a stroke.
Radiological findings
Patients with RCVS may present three types of stroke (convexity subarachnoid haemorrhage,
intracerebral haemorrhage,
and cerebral infarction) and reversible brain edema (Fig.16)
A combination of lesions can be present,
and different types of lesions can develop successively.
If the initial head CT findings are normal haemorrhage or infarctions may develop during the course of illness.
Vascular imaging findings may be evident on DSA CTA,
MRA...
and include multifocal segmental constrictions alternating with focal dilations or normal calibre vessels in multiple vascular distributions.
The vascular abnormalities typically resolve in 3 months.
Initial vascular imaging findings may be normal,
with abnormalities developing during days to weeks.
Thus,
despite normal angiography findings the diagnosis of RCVS must be considered in the appropriate clinical setting.
Prognosis
Timely diagnosis and treatment can potentially minimize the complications of the disease.
The most serious complications of RCVS are permanent neurological deficit and death.
Despite this,
the rate of permanent neurological disability is surprisingly low
The most common complications are ischemic infarcts,
convexity subarachnoid haemorrhage,
lobar intracerebral haemorrhage and cerebral edema
Cerebral infarction and intracerebral haemorrhage are predictors of a worse outcome.
Deaths from RCVS have been reported in the literature but are rare.













