IDENTIFY MEDIASTINAL MASSES
The first step in addressing mediastinal masses is suspect their mediastinal origin.
Radiographic features of a lesion of mediastinal origin are: The intimate effect of the mass with mediastinal structures,
smooth and sharp margins and obtuse angles between the mass and lung (1) (6)
Signs of the intimate effect of mediastinal structures are the change in the anatomy and movement of mediastinal structures adjacent to the injury,
displacement of the trachea,
main brochus or displacement of the heart.
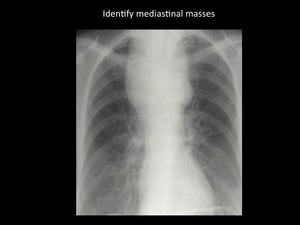
Fig. 2: Identify mediastinal origin. Chest radiography showing a mass in the upper third of the thorax, intimate effect with mediastinal structures is noted, with displacement of the trachea and smooth, sharp margins with obtuse angles. Patient with histological diagnosis of thyroid carcinoma. / Department of imaging - Santa Fé de Bogotá. Universitary Hospital.
Compartments and mediastinal anatomy
There are different anatomical classifications to divide the mediastinal compartments.
The most frequently used include models with three and four compartments.
The models are Felson model,
which is the same as the classification of Zylak,
the fleishner model,
the classification of Burkell,
the anatomical model and the model proposed by the Japanese Association for Research thymus (JART).
The Fleishner model,
the anatomical classification and the JART classification divide mediastinum in 4 compartments,
while Burkell and Felson modell divide mediastinum in 3 compartments.
The three-compartment model (Felson model) is going to be used throughout this chapter because it results the simpler model for a semiotic approach.
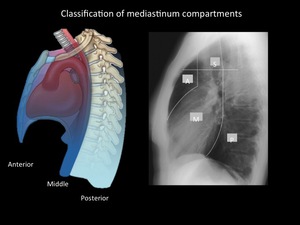
Fig. 3: Felson model (left), is a radiological classification and divide mediastinum into 3 compartments. This model uses as reference the lateral chest radiograph. The anterior mediastinum is bounded by an imaginary line from the upper thoracic inlet to the diaphragm delimited by the anterior edge of the heart and trachea, separating the anterior and middle mediastinum. The posterior mediastinum is formed on the back line of the trachea and heart to a line located one after the anterior margin of the vertebral bodies cm. In the Fleishner model (Right) 4 mediastinal compartments are included. In this classification there are upper and lower mediastinum. / Department of radiology - Santa Fé de Bogotá. Universitary Hospital.
Mediastinal compartments limits
| Compartment |
Limits |
Anatomical structures |
| Anterior |
Anterior: Sternum
Posterior: Anterior margin of pericardia,
aorta y brachiocephalic vessels.
Lateral: parietal pleura of both lungs. |
Timus
lymphatic nodes
Mediastinal fat
Internal mammary vessels |
| Middle |
Anterior: Anterior margin of pericardia,
aorta and brachiocephalic vessels.
Posterior: Posterior pericardia and great vessels.
Lateral: parietal pleura of both lungs. |
Heart and pericardium
Ascending and transverse aorta
Brachiocephalic vessels
Superior and inferior vena cava
Major pulmonary vessels
Trachea and main bronchi
Lymph nodes
Mediastinal Fat
|
| Posterior |
Anterior: Posterior pericardia.
Posterior: thoracic vertebral body.
(1 cm)
Lateral: parietal pleura of both lungs. |
Descending aorta
Esophagus
Thoracic duct
Azygos vein or hemiazygos
Autonomic nerves
Lymph nodes
Fat
|
Reviewed semiology of mediastinal lines,
bands and interfaces
A line is a longitudinal opacity of no more than 2mm wide.
The lines are posterior union line,
anterior union line and the right and left paraspinal lines.
They are formed by the close apposition of parietal and visceral pleura and the apposition of pleura and the side margins of the vertebral bodies respectively.
A band is a longitudinal opacity of major width.
Usually 2-5 mm wide.
The bands are right and left paratracheal stripes and are formed by the apposition of the pleura of the upper lobes and the side walls of the trachea.
An interface is formed apposition two tissues of different densities,
such as the lungs and heart.
Azigo – esophageal interface and the interface of the descending aorta are interfaces of mediastinum.
Mediastinal line,
band or interface displacement,
widening or abnormal contour are important signs of mediastinal pathology.
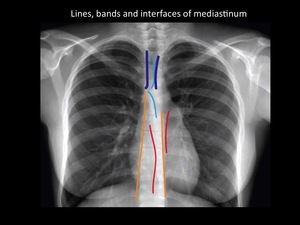
Fig. 4: Chest radiography scheme with lines, bands and interfaces. Representation of superior-posterior and inferior-anterior junction lines (Soft Blue); paraspinal lines (yellow), paratracheal bands (Dark blue) and azygo-aesophaeal and paraortic interfaces (Red). Department of diagnostic imaging - Santa Fé de Bogotá foundation.
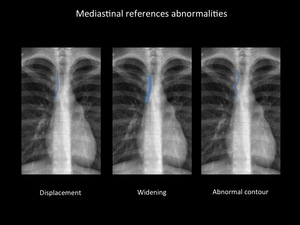
Fig. 5: Mediastinal line, band or interface displacement, widening or abnormal contour are important signs of mediastinal pathology. Department of diagnostic imaging - Santa Fé de Bogotá foundation.
MEDIASTINUM RADIOLOGICAL SEMIOLOGY REVIEWED
ANTERIOR MEDIASTINUM
The most frequent mediastinal semiology references in this compartment are: Alteration of the anterior junction line and the hilium overlay sign.
Anterior junction line
Anterior junction line is formed above the apposition of 4 layers of pleura in the anterior portion of the lung; 2 layers of visceral pleura and 2 layers of parietal pleura.
It is formed behind the upper two thirds of the sternum with an oblique orientation from top right to left bottom.
It is displayed in the 24 to 50% of plain radiography,
it’s viewing is facilitated on patients with pneumothorax and emphysema by lung hyperaeration.
It may disappear or have focal or diffuse thickening in patients with anterior mediastinal masses and their contours can be altered in endothoracic goiter,
thymoma,
neoplasms germ cells,
parathyroid adenoma,
lipomatosis,
lymphadenopathy,
pericardial cysts,
sternal hematomas and mediastinitis (3)(18).
In adults,
the anterior mediastinal masses are at highest risk of malignancy.
Approximately 56% of all anterior mediastinal lesions are malignant (19) (20).
The most frequent masses in the anterior mediastinum are thymic masses and thyroid masses.
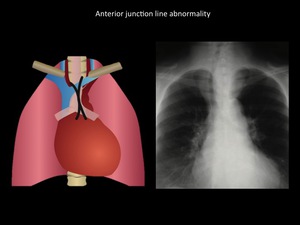
Fig. 6: (Left) Scheme showing normal anterior junction line location (Right) Mass in the upper third of the mediastinum, with effacement of the anterior junction line, displacement of the trachea to the right and clear interface with the lung, clearly representing a mediastinal mass. Patient diagnosed with intrathoracic goiter. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary hospital.
Hilar overlay sign
It is useful to distinguish a non-hilar from an hilar mass.
It allows locating a mass in the anterior or posterior mediastinum.
If we visualize the vessels of the hilium through the mass,
means that the mass is not born of the hilum and therefore will be located in the anterior or posterior mediastinum.
Most of these masses will be located in the anterior mediastinum (9).
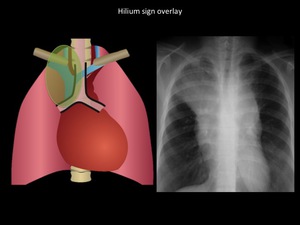
Fig. 7: Illustration shows parahiliar (Paratracheal) lines. Chest radiograph demonstrates a well defined borders mass located in the upper third of the mediastinum, hilium overlay sign and disappearance of anterior junction line. Patient was diagnosed with thymic carcinoma. Hilum overlay sign differentiates the anterior or posterior mediastinal masses from the middle mediastinum masses. The anterior mediastinal or posterior mediastinal masses overlay the hiium without displacing it. In adults the masses of the anterior mediastinum have a higher risk of malignancy than the rest of the mediastinum; 56% of all lesions of the anterior mediastinum are malignant. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.
Cervicothoracic sign
The anterior mediastinum ends at the superior aspect of the clavicle and the posterior mediastinum ends above the level of the clavicles.
When a mass projects above the clavicles it is likely be located in the posterior mediastinum or cervical structures (18).
Additionally,
the supraclavicular masses outside the mediastinum,
have no clear interface with the lung and have not well defined margins,
while mediastinal supraclavicular masses located in the posterior mediastinum have a well defined interface with the lung and their margins are better defined.
There is no middle mediastinum masses above clavicles.
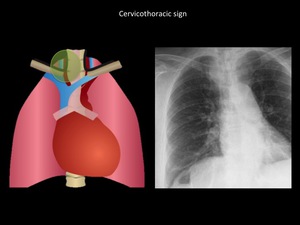
Fig. 8: Mass that projects above right clavicle, with clear interface with the lung and well defined margins. Endothoracic goiter was confirmed. When a mass projects above the clavicles it is likely be located in the posterior mediastinum or cervical structures. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.
Silhouette sign
The silhouette sign means that masses of similar density when are in contact lose the delimitation of its borders.
The masses in contact with the edge of the diaphragm or pericardium will have little distinguishable edges.
In the mediastinal pathology,
injuries that have this sign are in most of time lipomas,
pericardial cysts and hernias of Morgagni.
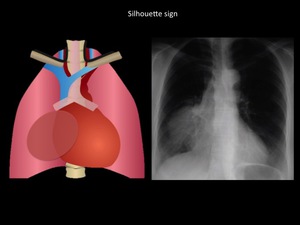
Fig. 9: Parahilar right homogeneous mass with well-defined edges, in contact with the diaphragm, and making silhouette sign with mediastinum. Patient with thymic carcinoma. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.
MIDDLE MEDIASTINUM
Mediastinal lesions can manifest as opacification of aorto pulmonary window and alteration of the left or right paratracheal stripe.
The presence of lymphadenopathies,
mediastinal widening and changes in the orientation of the trachea always orientate to alterations of middle mediastinum.
Aorto pulmonary window
It is the concavity formed between the aortic arch and the left pulmonary artery.
It is bounded by the parietal pleura laterally and medially by the arterial ligament.
Their normal appearance is a concavity.
It is usually visible in the majority of chest radiographs.
May become convex if there are lymphadenopathies,
enlargement of the ductus arteriosus and aortic aneurysms.
The shape of the aortopulmonary window can be altered by anterior mediastinal masses,
posterior compartment masses,
and tumors of the nerve sheath of the recurrent laryngeal and the left vagus nerves.
In diaphragmatic paralysis or paralysis of the left vocal cord must be properly assess the aortopulmonary window,
to rule out laryngeal nerve and vagus nerve tumors (2) (3) (21).
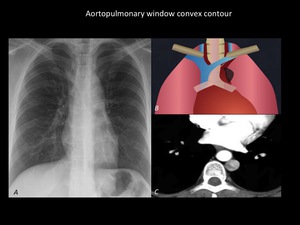
Fig. 10: Chest radiograph (A) and Illustration (B) demonstrate convex contour of aortopulmonary window which is considered abnormal. CT scan (C) reveals the presence of left superior vena cava as a anatomical variant. The mediastinal masses of the anterior compartment or nerve sheath tumors of recurrent laryngeal nerve and left vagus nerve can also alter the contour of the aortopulmonary window. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.
Right paratracheal band
It is one of the anatomical references that more is viewed on the chest radiograph,
being present up to 97% of all radiographs (9).
The right paratracheal stripe is formed by the tracheal wall,
the adjacent tissue and mediastinal pleura of the right lung.
Its normal thickness is 1-4 mm and is in close relationship with the azygos vein.
It is the line most associated with match effect.
The paratracheal stripe thickening can occur to the mediastinal lipomatosis,
lymphadenopathy,
masses or tracheal bleeding.
In the history of trauma,
the display line can rule right paratracheal mediastinal hematoma and injury of large vessels (22).
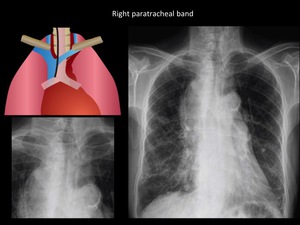
Fig. 11: Predominantly right thickening of both paratracheal bands, suggestive of middle mediastinum disease. Asociated paratracheal lymphadenopathy is viewed. Small cell type lung carcinoma was confirmed. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.
Left paratracheal stripe
It is formed by the contact of the left lung,
the left tracheal wall and the adjacent mediastinal soft tissue,
it is placed over the aortic button under the superior thoracic inlet.
It may be a line or a band and its visualization is rare,
being present only in 21-31% of the radiographs (3,23,24),
so its widening can be difficult to diagnose.
In a manner similar to the right paratracheal stripe,
the presence of osteophytes,
medistinal lipomatosis or bleeding can alter their appearance.
The tortuosity of the aorta can also move this band.
Mediastinal widening
The mediastinal widening is defined as the widening of the mediastinum more than 8 cm at the height of the of the thoracic aorta button (25).
It is one of the most common signs of mediastinal disease,
occurring in approximately 77% of patients with mediastinal lesions (19).
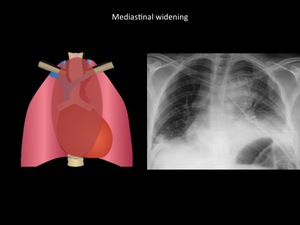
Fig. 12: Mediastinal widening and bilateral pleural effusions in patient with history of posterior mediastinal resection of mediastinal tumor and posterior bleeding. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary Hospital
Lymphadenomegaly
The differential diagnosis of lymphadenopathy is broad.
44% of mediastinal lesions have in their presentation lymphadenopathies and may or may not be associated with broadening and disappearance of the paratracheal lines.
The presence of lymphadenopathy is the most common presentation in primary mediastinal lymphoma or mediastinal extension of lung cancer or lymphoma.
The finding of calcified lymphadenopathy "eggshell" is very common in advanced stages of silicosis,
however its not unique and specific for this disease and may be present in diseases like sarcoidosis,
nodal and lung disease of tuberculosis and post irradiation Hodkin lymphoma.
The sensitivity and specificity of radiography for detecting lymphadenopathy in patients with tuberculosis is moderate,
being less sensitive in the pediatric population.
When is used the lateral radiograph additionally to anteroposterior projection,
it does not increase the diagnostic accuracy of detecting lymph node enlargement (26).
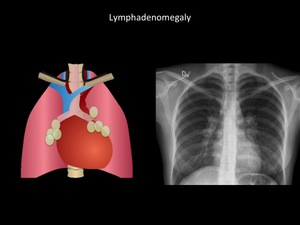
Fig. 13: Thickening of both paraspinal lines, multiple lymphadenopathy (compromise of middle mediastinum). Sarcoidosis was confirmed
Deviation of the trachea
The deviation of the trachea is a useful sign and it is founded more frequent in the middle mediastinum injuries.
In elderly patients physiological deviation of the lower third of the trachea can be a normal finding (9).
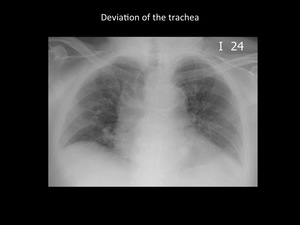
Fig. 14: Significant right deviation of the trachea secondary to ascending aorta aneurysm. Bilateral alveolar opacities by multilobar pneumonia. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary Hospital
The deviation of the trachea is a common finding,
being an incidental finding as much as 37% of patients,
however,
this finding in the preoperative context,
is not related to difficulties in intubation or increase in the number of intubation attempts (36).
Tracheal deviation despite being a prominent finding in the mediastinal semiotics,
has been found more related to benign diseases,
such as intrathoracic goite, that malignant diseases (39) (40).
POSTERIOR MEDIASTINUM
Paraspinal lines
Paraspinal lines are interfaces between the medial portions of the back lobes and paraspinal tissues of the column.
They are abnormal when become ticked, have distortions or disruptions in continuity.
The left paravertebral line is usually visible under the aortic arch,
extending vertically parallel to the spine to the left diaphragmatic crus.
It is observed in midway between the spine and the lateral margin of the aorta.
Right paravertebral line is thinner than the line paravertabral left and thus less visible.
It is observed only in its portion adjacent to the lower vertebrae of the thoracic spine,
where converges vertically to the right diaphragmatic crura.
It is usually viewed through or adjacent to the air column of the trachea.
(23)
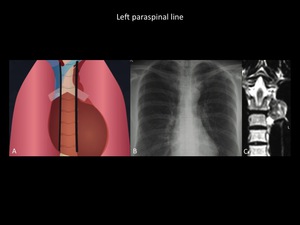
Fig. 15: Illustration (A) of normal paraspinal lines. Chest radiograph (B) demonstrates well defined mass in the upper left mediastinum third, which is projected over the aortic arch, originated from the left paraspinal line. Coronal T2 MRI (C) shows the same left paravertebral mass, which has an heterogeneous signal intensity in a patient with extramedullary hematopoiesis. The left paraspinal line is more frequently seen than the right line. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary Hospital
Processes that affect the diameter and course of the thoracic aorta usually alter the left paravertebral line.
The most common cause of thickening of the right paravertebral are osteophytes (23).
The pathologies that can affect both paravertebral lines are the spinal trauma,
pleural effusion,
the lymphadenopathy,
vertebral and paravertebral disorders,
paravertebral masses and subsequent widening of veins and azygos hemiazygos.
Para-aortic line
It is a line that is best viewed in the lateral projection.
It is the line that forms from the contact between the descending aorta and the medial aspect of the left lower lobe,
it has a parallel orientation to the paraspinal line; is often displayed on chest radiographs and it is accented in cases of dorsal kyphosis,
tortuosity of the aorta and emphysema (9).
The displacement of the aortic button on more than 10 mm,
measured from the middle of the circumference of the aortic button to the left side of the trachea (see figure) has a moderate sensitivity and specificity (78% and 78% respectively) for the diagnosis of a left paratracheal esophageal mass (44)
Posterior junction line
It is formed by the contact between the back portions of the lung in the upper mediastinum.
It is posterior to esophagus and anterior to the upper thoracic vertebral bodies.
It is a union that forms from the apposition of 4 layers of pleura (2 parietal visceral and 2) and a variable amount of fat.
Usually it is a straight or slightly concave line.
It is commonly viewed and can be altered in the presence of esophageal abnormalities or masses at this location (23).
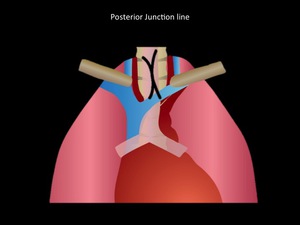
Fig. 16: Posterior junction line scheme. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary Hospital
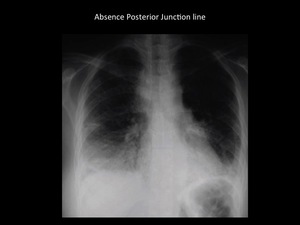
Fig. 17: Mediastinal widening, bilateral pleural effusions and absence of posterior junction line in patient diagnosed with retropharyngeal mediastinitis access. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary Hospital
Azygous Esophageal recess
The Azygous Esophageal recess is a mediastinal interface caused by the different densities between the mediastinum and the posteromedial portion of the right lower lobe.
This represents the space between the side or rear wall of the middle and lower third of the esophagus and the pleura anterior to the vertebral bodies,
extending from the arch of the azygos vein to the aortic hiatus (3).
The Azygo-oesophageal recess is often visualized on plain radiographs as an "inverted S" presenting slight convexity to the left in the top segment with a lower straight edge; the upper right convexity can be seen in children and young adults,
but it is abnormal in older adults,
suggesting pathology in this location (3) (7).
Such mediastinal interface,
can occur in 21% of patients in a concave shape without represent pathological changes (46)
The displacement of the ácigo-esophageal recess may occur in cases of loss of lung volume with partial or complete collapse of the lower lobe,
esophageal dilation,
abscess or mediastinal masses (7).
An abnormal contour of this line may be due to lymphadenopathy,
hiatal hernias,
bronchopulmonary malformations,
esophageal neoplasms,
pleural abnormalities and cardiomegaly with dilatation of the left atrium (3).
MEDIASTINAL PATHOLOGY
Mediastinal masses are a common finding on chest radiograph,
and most of them are incidental.
The relative frequency of mediastinal lesions is difficult to estimate because many of the series of cases are based on patients who are taken to biopsy or surgical resection (47) rather than the radiological findings.
Approximately 75% of all mediastinal lesions are benign lesions and 25% are malignant,
unresectable lesions.
Including pediatric and adult population and all mediastinal compartments,
80% of mediastinal lesions are thymic neoplasms (thymoma,
thymic carcinoma),
thyroid goiter and esophageal masses.
Thymic and thyroid lesions are more common in the adult population (48) and neurogenic tumors,
germ cell tumors and cysts of foregut represent 80% of mediastinal masses in children (24).
Lymphoma and mediastinal cysts have a similar prevalence in the pediatric population than in the adult.
Mediastinal masses are more frequent in males (19),
with a ratio of male to female of about 2: 1.
The percentage of benign lesions varies with the age of patients,
the most frequent malignant occur in older ages.
Benign lesions are slightly more frequent in the 3rd and 4th decade of life.
Primary mediastinal tumors are rare tumors,
representing approximately 3% of all tumor lesions of the chest (51) (19) (52).
The most common site of mediastinal masses is the anterior chamber,
followed by the middle mediastinum and the multi-compartment location.
(20).
Benign lesions are less frequent in the posterior mediastinum and more frequent in the anterior mediastinum.
The large variation in the distribution of mediastinal lesions in the different series of cases depends on the inclusion of the pediatric population and the inclusion of mediastinal lesions with extension to mediastinal compartments as bronchogenic carcinoma,
lymphoma and tuberculosis (53).
In the anterior compartment,
the probability of an etiologic diagnosis based on the appearance of the lesion is approximately 36% for plain radiography and 48% for contrasted tomography.
When taking into account only the three most common differential diagnoses,
the probability of an etiologic diagnosis only with images increases to 59% for plain radiography and 72% for contrasted tomography respectively (58).


, is a radiological classification and divide mediastinum into 3 compartments. This model uses as reference the lateral chest radiograph. The anterior mediastinum is bounded by an imaginary line from the upper thoracic inlet to the diaphragm delimited by the anterior edge of the heart and trachea, separating the anterior and middle mediastinum. The posterior mediastinum is formed on the back line of the trachea and heart to a line located one after the anterior margin of the vertebral bodies cm. In the Fleishner model (Right) 4 mediastinal compartments are included. In this classification there are upper and lower mediastinum. / Department of radiology - Santa Fé de Bogotá. Universitary Hospital.")
; paraspinal lines (yellow), paratracheal bands (Dark blue) and azygo-aesophaeal and paraortic interfaces (Red). Department of diagnostic imaging - Santa Fé de Bogotá foundation.")

 Scheme showing normal anterior junction line location (Right) Mass in the upper third of the mediastinum, with effacement of the anterior junction line, displacement of the trachea to the right and clear interface with the lung, clearly representing a mediastinal mass. Patient diagnosed with intrathoracic goiter. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary hospital.")
 lines. Chest radiograph demonstrates a well defined borders mass located in the upper third of the mediastinum, hilium overlay sign and disappearance of anterior junction line. Patient was diagnosed with thymic carcinoma. Hilum overlay sign differentiates the anterior or posterior mediastinal masses from the middle mediastinum masses. The anterior mediastinal or posterior mediastinal masses overlay the hiium without displacing it. In adults the masses of the anterior mediastinum have a higher risk of malignancy than the rest of the mediastinum; 56% of all lesions of the anterior mediastinum are malignant. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.")


 and Illustration (B) demonstrate convex contour of aortopulmonary window which is considered abnormal. CT scan (C) reveals the presence of left superior vena cava as a anatomical variant. The mediastinal masses of the anterior compartment or nerve sheath tumors of recurrent laryngeal nerve and left vagus nerve can also alter the contour of the aortopulmonary window. Department of diagnostic imaging. Santa Fé de Bogotá foundation. Universitary hospital.")


. Sarcoidosis was confirmed")

 of normal paraspinal lines. Chest radiograph (B) demonstrates well defined mass in the upper left mediastinum third, which is projected over the aortic arch, originated from the left paraspinal line. Coronal T2 MRI (C) shows the same left paravertebral mass, which has an heterogeneous signal intensity in a patient with extramedullary hematopoiesis. The left paraspinal line is more frequently seen than the right line. Department of diagnostic imaging - Santa Fé de Bogotá foundation. Universitary Hospital")

