ECR 2017 / C-1894
Müller Weiss Syndrome: a forgotten cause of mid foot pain. A multimodality pictorial review.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-1894
Type:
Educational Exhibit
Keywords:
Musculoskeletal bone, Extremities, Bones, Fluoroscopy, CT, MR, Diagnostic procedure, Trauma, Developmental disease, Ischaemia / Infarction
Authors:
A. Fuentealba, S. Butrón, J. Drewes, N. Rossel, J. P. Durán, A. J. Provoste Soto, M. CASTRO; Santiago/CL
DOI:
10.1594/ecr2017/C-1894
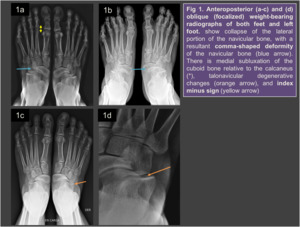
 and (d) oblique (focalized) weight-bearing radiographs of both feet and left foot. References: Department of Radiology, Clínica INDISA; Santiago, Chile")
Fig. 1:
Fig 1. Anteroposterior (a-c) and (d) oblique (focalized) weight-bearing...

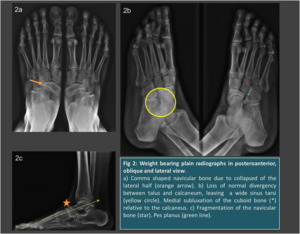
Fig. 2:
Fig 2: Weight bearing plain radiographs in posteroanterior, oblique and lateral...
 References: Department of Radiology, Clínica INDISA; Santiago, Chile")
Fig. 3:
Fig 3: Radiographs of both feet in oblique views (a-b)

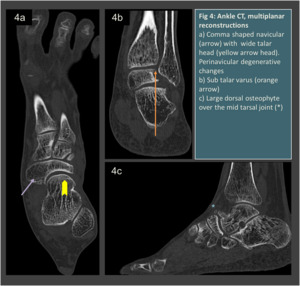
Fig. 4:
Fig 4: Ankle CT, multiplanar reconstructions
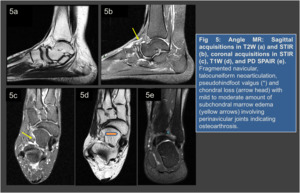
 and STIR (b), coronal acquisitions in STIR (c), T1W (d), and PD SPAIR (e) References: Department of Radiology, Clínica INDISA; Santiago, Chile")
Fig. 5:
Fig 5: Angle MR: Sagittal acquisitions in T2W (a) and STIR (b), coronal...
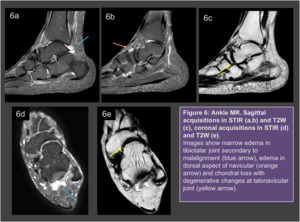
 and T2W (c), coronal acquisitions in STIR (d) and T2W (e) References: Department of Radiology, Clínica INDISA; Santiago, Chile")
Fig. 6:
Figure 6: Ankle MR. Sagittal acquisitions in STIR (a,b) and T2W (c), coronal...