Introduction:
Achalasia is a primary neurological esophageal motor disorder,
characterized by the absence of primary peristalsis and incomplete or absent relaxation of lower esophageal sphincter (LES) with swallowing,
and normal or abnormal high resistance LES pressure.
It is the most common esophageal motor disorder,
with mean incidences of 0.3-1.63 per 100 000 people per year in adults,
it occurs with equal distribution in men and women with a bimodal distribution,
early onset at age 20 to 40,
and late onset after age 60.
The clinical syndrome occurs because of ganglion cells loss in the intermyenteric (Auerbach´s) plexus,
neurons that elaborate inhibitory neurotransmitters,
such as vasoactive intestinal polypeptide and neuropeptide Y and respective neurotransmitters are decreased in the lower esophagus in these patients,
but the etiology of these neuronal changes remains unknown.
The common symptoms at the time of presentation are dysphagia (>90%) for solids and liquids,
chest pain (vigorous achalasia),
delayed regurgitation of undigested foods,
weight loss,
vomiting,
and reflux which appear insidiously.
And it can be assessed with the Eckart score (Fig. 2),
high scores are associated with treatment failures.
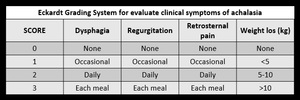
Fig. 2: Eckardt Grading System for evaluate clinical symptoms of achalasia.
References: Eckardt VF, Aignherr C, Bernhard G. Predictors of outcome in patients with achalasia treated by pneumatic dilation. Gastroenterology. 1992;103:1732-38
Diagnostic:
The first diagnostic step is to rule out anatomical lesions (pseudoachalasia) using endoscopy or radiology.
Endoscopy allows inspection of the esophageal mucosa and shows retained food and superficial ulcerations of the mucosa.
Typically,
the endoscope can pass through the cardia,
unlike with other obstructive organic entities (carcinoma,
or peptic strictures).
The radiologic examination is important to rule out structural abnormalities,
and to estimate the esophageal diameter.
Barium swallow is the method of choice in these patients and is performed under fluoroscopic guidance.
A normal exam does not exclude achalasia,
especially in early stages,
where manometry is mandatory.
In affected individuals show absence of peristalsis in the esophagus body which is dilated and tortuous,
retention of contrast above the LES,
and the distal portion has a characteristic appearance of a cone (bird´s beak) (Fig. 3).
To assess emptying of the esophagus,
a timed barium esophagogram (TBE) can be done,
in which the height of the barium column is measured,
as it empties during the 1st,
3rd and 5th min after the ingestion of diluted barium.
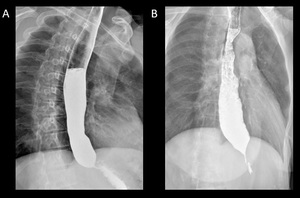
Fig. 3: Barium swallow images in patients with achalasia shows esophageal dilatation, narrowing of distal esophagus with classic bird´s beak tapering at the LES, and loss of peristalsis in the distal two thirds.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
The gold standard for diagnosis is manometry,
which makes an objective measurement of esophageal contractility and demonstrates:
• Normal function of the cricopharyngeal sphincter.
• Absence of primary peristalsis in the body of the esophagus.
• Simultaneous and discordant contractions.
• High pressure in the LES (usually double than normal = 40 mmHg).
• Absent or incomplete relaxation after swallowing
• Phenomena typical of other swallowing disorders such as diffuse spasm,
large amplitude peristaltic waves,
etc.,
can also be observed in some patients.
Three distinct subtypes of achalasia (types I,
II,
and III) are defined with high-resolution manometry (Fig. 4) that have both prognostic and potential therapeutic implications.
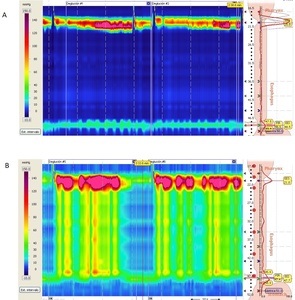
Fig. 4: High-resolution Manometry in patients with achalasia. A) Manometry in a Type I achalasia shows impaired LES relaxation, absent peristalsis, and normal esophageal. B) Manometry in a type II achalasia shows impaired LES relaxation, absent peristalsis, and increased pan-esophageal pressure.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Normal anatomy:
Studies of the esophagus consist of single-contrast,
double-contrast,
and mucosal relief views,
together with fluoroscopic evaluation of motility.
Normal esophageal tonicity leads to lumen collapse when a primary peristaltic wave has passed.
Therefore,
the study must be performed reasonably quickly.
Full-column images of the esophagus are usually obtained with the patient on the fluoroscopic table in the prone,
right anterior oblique position.
Esophageal peristalsis is inhibited by rapid swallowing of barium,
allowing the esophagus to distend fully.
The normal distended esophagus has a thin white luminal contour in profile and a smooth homogeneous appearance en face.
Collapsed or partially collapsed views (mucosal-relief views) show the normal longitudinal folds as thin,
straight,
delicate structures no more than 1–2 mm in width (Fig. 5).
Fig. 5: Barium swallow showing normal anatomy of esophagus. The normal distended esophagus has a thin white luminal contour in profile and a smooth homogeneous appearance en face.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Time barium esophagogram:
In a person with normal esophageal function,
the esophagus should be emptied of 250 mL of barium within 10 to 20 seconds and must have no residual barium after 1 minute.
In achalasia patients have a massively dilated esophagus and the emptying is delayed.
TBE is specifically performed to evaluate esophageal emptying.
Its potential advantage is that it offers dynamic information and standardized assessment of the esophagus,
quantifying esophagus emptying easily and accurately.
It is easily performed,
inexpensive,
quantitative,
repeatable,
and comfortable for the patient.
Now is used to evaluate response to pneumatic dilation or surgery.
TBE technique:
The technique is like a typical barium swallow with some modifications.
The examination is performed in the upright left posterior oblique position after fasting,
the patient is instructed to drink up to 250 mL of low-density barium sulfate suspension within 30 to 45 seconds (the volume of suspension should be such that patient can tolerate it well without regurgitation or aspiration.
Three-on-one spot films of the esophagus are taken at 1,
2 and 5 min after the start of the barium ingestion (Fig. 6,
Fig. 7). The distance between the fluoroscope carriage and the patient is kept constant during all three spot films.
For sequential studies before and after treatment for achalasia,
the same volume of barium as ingested for the baseline examination must be used to have consistent results.
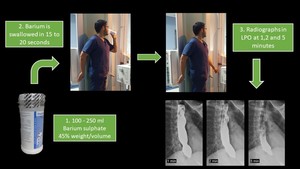
Fig. 6: Time barium esophagogram technique. The patient is instructed to drink up to 250 mL of low-density barium sulfate suspension within 30 to 45 seconds. Three-on-one spot films of the esophagus are taken at 1, 2 and 5 min after the start of the barium ingestion.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Fig. 7: Time barium esophagogram. Videofluoroscopy showing the patient ingesting 250 ml of low density barium contrast in approximately 20 seconds.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX



 Manometry in a Type I achalasia shows impaired LES relaxation, absent peristalsis, and normal esophageal. B) Manometry in a type II achalasia shows impaired LES relaxation, absent peristalsis, and increased pan-esophageal pressure. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")


