ECR 2018 / C-2303
Patent paraumbilical vein on ultrasound: not always cirrhosis
Congress:
ECR 2018
Poster Number:
C-2303
Type:
Educational Exhibit
Keywords:
Tropical diseases, Connective tissue disorders, Cirrhosis, Education, Ultrasound-Spectral Doppler, Ultrasound-Colour Doppler, Ultrasound, Veins / Vena cava, Liver, Abdomen
Authors:
J. C. Nogueira Junqueira1, A. Cavalanti1, M. C. Chammas1, H. Durante2, S. M. Ando1; 1São Paulo/BR, 2SÃO PAULO, SP/BR
DOI:
10.1594/ecr2018/C-2303

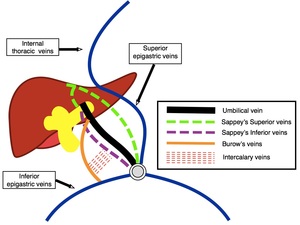
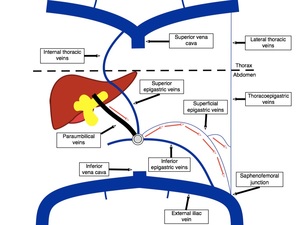
Fig. 1:
Simplified scheme demonstrating the umbilical vein and the paraumbilical veins.

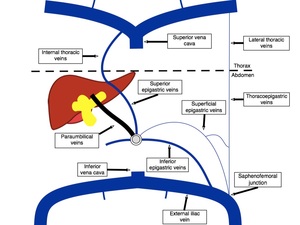
Fig. 2:
Simplified scheme demonstrating the paraumbilical veins and their main venous...

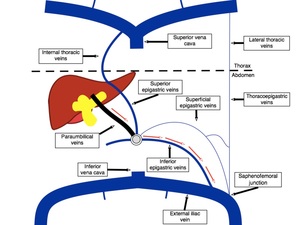
Fig. 3:
Simplified scheme demonstrating hepatofugal flow through the paraumbilical...

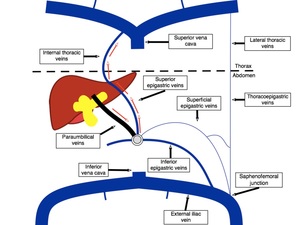
Fig. 4:
Simplified scheme demonstrating hepatofugal flow through the paraumbilical...

Fig. 5:
Simplified scheme demonstrating hepatofugal flow through the paraumbilical...
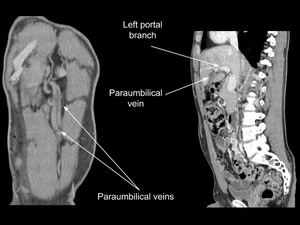
 images from enhanced abdominal CT showing patent paraumbilical veins and their communication with the left branch of the portal vein in a patient with extensive inferior vena cava (IVC) thrombosis. References: Institute of Radiology (InRAD), Hospital das Clínicas, University of São Paulo (USP)/ Brazil 2018.")
Fig. 6:
Coronal and sagittal multiplanar reformation (MPR) images from enhanced...
, Hospital das Clínicas, University of São Paulo (USP)/ Brazil 2018.")
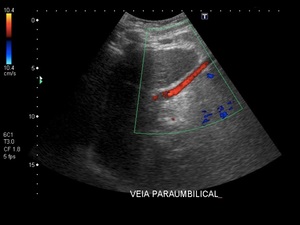
Fig. 7:
Ultrasound Doppler image of a typical patent paraumbilical vein with...
, Hospital das Clínicas, University of São Paulo (USP)/ Brazil 2018.")
Fig. 8:
Ultrasound Doppler image of a typical patent paraumbilical vein with...
. References: Institute of Radiology (InRAD), Hospital das Clínicas, University of São Paulo (USP)/ Brazil 2018.")
Fig. 9:
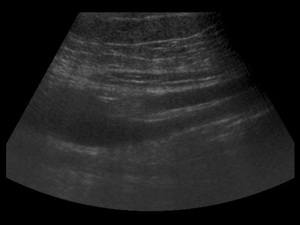
Ultrasound image of two paraumbilical veins posterior to the rectus sheath...
. Because of their tortuosity, they simulate the existence of four veins. References: Institute of Radiology (InRAD), Hospital das Clínicas, University of São Paulo (USP)/ Brazil 2018.")
Fig. 10:
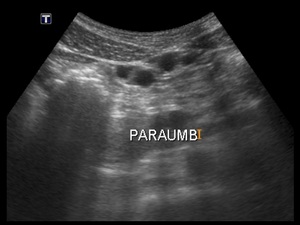
Ultrasound image of two paraumbilical veins posterior to the rectus sheath...
 and transverse image of two paraumbilical veins posterior to the rectus sheath, simulating the existence of four veins, because of their tortuosity (images on the right). References: Institute of Radiology (InRAD), Hospital das Clínicas, University of São Paulo (USP)/ Brazil 2018.")
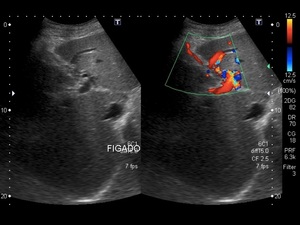
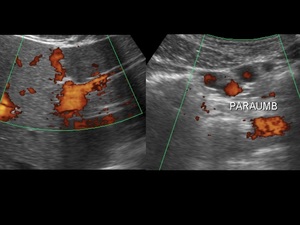
Fig. 11:
Ultrasound Power Doppler image of paraumbilical veins with their connection...