Type:
Educational Exhibit
Keywords:
Abdomen, Kidney, CT, MR, Ultrasound, Biopsy, Cancer, Cysts
Authors:
A. Patel1, G. Chow2, R. Vaja3, C. King1, S. chang1; 1Stevenage/UK, 2London/UK, 3CB2 0SP/UK
DOI:
10.1594/ecr2018/C-2392
Conclusion
The exponential growth of cross-sectional imaging has significantly contributed to a similar rise in the detection of incidental renal lesions.
Small indeterminate renal lesions on conventional abdominal CT (portal venous phase) should be carefully compared to previous available imaging or undergo further imaging characterisation with focused ultrasound,
multi-phase renal CT or contrast-enhanced MRI as proposed in figure 11.
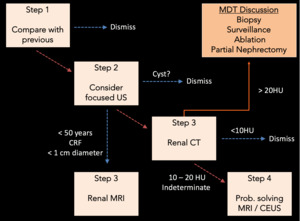
Fig. 11: Proposed algorithm for the diagnostic work up of an indeterminate renal lesion detected on conventional portal venous phase abdominal CT.
On multi-phase CT,
a contrast enhancement gradient of ≥ 20 HU signifies solid vascularised tissue compatible with a primary renal lesion.
Benign lesions also demonstrate variable contrast enhancement and represent up to 20% of resected lesions <4 cm.
Indeterminate lesions on CT (enhancement gradient 10-20 HU) should ideally undergo further imaging assessment with CEUS or MRI.
Alternatively for selected patients (for example an elderly patient with other more significant co-morbidities),
imaging surveillance to assess for interval growth is also acceptable.
Percutaneous biopsy should be considered for lesions remaining indeterminate after all imaging modalities have been exhausted. Biopsy prior to percutaneous ablation is essential in order to prevent unnecessary treatment of histologically benign lesions.

