MUSCLE INJURIES
Muscle injuries are inevitable complications of physical activity,
particularly in elite athletes submitted to high loads of forces during their activity.
They have an important physical and economic impact for the athlete,
but also affect the coach,
the entire team and the fans.
Imaging techniques assume a pivotal role in helping the clinician diagnose or confirm the injury,
determine its extent and severity.
Therefore,
they are an important tool for the physician to establish the best time to come back to training and competition,
reducing the risk of recurrence.
Imaging is also important to assess healing and exclude complications.
Although MRI has been considered the gold standard technique,
Ultrasound (US) has assumed a popular acceptance as the first and,
sometimes,
the only imaging technique needed to complement the physical exam.
Its availability and low cost make it an attractive tool for this purpose.
Moreover,
it’s a fast and inexpensive exam,
allows a multiplanar approach,
a dynamic examination of the muscle during rest and contraction,
has an excellent spatial resolution (better than MRI) and the ability to study the lesion vascularization without contrast agents.
Limitations of diagnostic ultrasound comprise its operator dependence and its decreased resolution for deeper structure,
that can become very relevant in deep muscular group lesions or obese patients.
Its smaller field-of-view compared to MRI can also limit the evaluation of the longitudinal extent of the lesion.
This problem can be overcome by the use of trapezoid and extended field-of-view.
US has also less contrast resolution compared to MRI and is thus less sensible for depicting small contusions that present with edema on MRI.
- US technique
Following an adequate clinical history and short physical examination,
the exam might be directed to the anatomical part of clinical suspicion.
The patient should be placed in a comfortable position,
allowing scanning of the muscles in question,
from the proximal to the distal attachments,
including dynamic evaluation if needed.
The symptomatic region as well as the entire muscle should be examined,
including the myotendinous and myofascial junctions.
The surrounding vascular and nervous structures must also be studied,
allowing a differential diagnosis and the assessment of complications.
Both transverse and longitudinal sonographic evaluations are mandatory.
Assessment of muscle injuries requires high frequency linear probes and,
in our hospital,
probes ranging from 6 – 17 MHZ are used.
The adequate probe and frequency to be used depends on the balance between signal penetration and resolution,
with the principle of choosing the highest frequency possible for a certain depth.
The focus should be placed slightly below the area of interest and multiple focus can be used to enhance the assessment of large areas with uniform resolution.
Harmonic imaging can be used to reduce artefacts,
which might be especially tailored to distinguish between solids and liquids (e.g.
Hematomas).
The extended or trapezoid field-of-view are used for large lesions,
creating an image that might be easier for the clinician to interpret (Fig.
1).
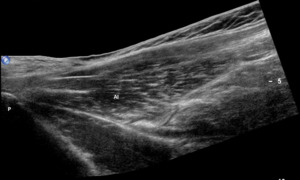
Fig. 1: Extended Field-of-view demonstrating the adductor longus in longitudinal section from its insertion in the superior pubic ramus. Al – Adductor longus; P – Pubis.
Both Power and Colour Doppler might be used in assessing tissue vascularity,
which might help identify the injury site (displaying increased vascularity),
and also distinguish between solid and liquid lesions.
It’s also useful in the healing evaluation (an hypervascularity means an active healing process).
Dynamic study is,
in certain cases,
very important,
allowing the detection of subtle tears not apparent during resting (video in image 2).
It also allows the detection of small muscular hernias.

Fig. 2: Small muscle tear in the long head of the biceps femoris, between this muscle and the semitendinous muscle, apparent only in the dynamic study with muscle contraction. lhBF –Biceps femoris long head; ST – Semitendinous muscle.
It´s especially important to avoid too much pressure,
as it can mask a small tear (Fig.
3).

Fig. 3: Small elongated fluid collection representing hematoma (arrowheads) indicating muscular tear in the adductor brevis. This highlights the importance of gente probe handling as increased probe pressure might cause the colapse of the fluid collection and a false negative result.
Finally,
comparison with the contralateral limb might be important for avoiding pitfalls.
- Time of examination
In the first 24-48 hours,
the hematoma is still in formation.
Its diffuse (not organized) location and hyperechogenicity might lead to false negative results.
After 48-72 hours,
hematomas will become well defined hypoechoic/anechoic fluid collection,
easily depicted on US.
For some authors,
the ideal time for the examination is between 2 and 48 hours after the traumatic event.
Before this period the hematoma is still in formation and after the second day the hematoma might spread outside the muscle if the aponeurosis is torn and might be harder to diagnose.
From our experience,
an ultrasound can be made in the first 24 hours,
but it can be important to repeat it after 48-72 hours to better assess the lesion extent.
Anyway,
time window can depend on the type of injury and the muscles affected.

