NORMAL MUSCLE
Muscle fibers are hypoechoic structures arranged in a parallel fashion and surrounded by hyperechoic fibroadipose septa called perimysium.
The epimysium is an hyperechoic fibrous fascia that envelops the entire muscle.
Fascia and tendons also appear hyperechoic compared to normal muscle (Fig.
4).
Fig. 4: Normal muscle structure structure with hypoechoic fibres arranged in a parallel fashion and surrounded by hyperechoic perimysium (arrows). The epimysium is an hyperechoic fibrous fascia that envelops the entire muscle (arrowheads).
PATHOLOGIC FINDINGS
Muscular injuries can be grouped in direct injuries,
occurring from a direct stress,
or indirect injuries,
which results from excessive load on the muscle,
usually leading to injuries at the weakest points (e.g.
the musculotendinous junction).
-Direct injuries
These injuries encompass laceration and contusion.
Laceration involves skin discontinuity and are not so common in sports activities.
Contusion is a non-penetrating injury caused by a direct impact.
These are more common in contact sports (e.g.
football and rugby).
The most involved muscles in the lower limbs are the quadriceps and gastrocnemius.
The diagnosis is mainly clinical,
but US is important to exclude an associated tear,
as well as to evaluate the extension and possible complications.
Clinically,
contusions result in localized pain,
stiffness and decrease in the range of motion.
A clinical grading of contusion can be established by the decrease in the range of motion from mild to severe.
The imaging appearance depends on the size and time elapsed since the event.
In the hyperacute phase (< 2h),
the muscle might appear swollen but with normal echogenicity.
After this period,
it presents as an area of hyperechogenicity surrounded by normal appearing fibres.
These findings may be similar to indirect lesions (grade 1 in Peetrons classification),
but may cross fascial planes,
unlike indirect injuries (Fig.
5).
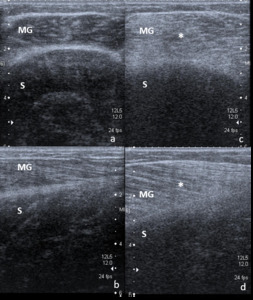
Fig. 5: Athlete with a direct posterior blow in the left calf during a football match. The right normal calf is shown in transverse and longitudinal planes (a and b, respectively). Increased thickness of the medial gastrocnemius is seen, showing an hyperechoic structure than can also be seen in the most superficial fibres of the soleus muscle, consistent with contusion (c and d in transversal and longitudinal sections, respectively). Note that the increased echo attenuation caused by the thickned gastrocnemius does not allow a proper evaluation of the soleus muscle, despite the low position of the focus (transverse sonogram in c). No signs of tear are identified. MG – Medial gastrocnemius; S – Soleus muscle.
If the force applied is substantial,
a muscle tear might result,
with hematoma formation.
In the first 24 hours,
the hematoma can have a varied appearance,
that ranges from anechoic/hypoechoic to hyperechoic.
After 48-72 hours this collection will appear as an hypoechoic/anechoic collection with irregular margins of muscle fibres.
The margins of the collection become well defined.
Progressively the margins “enlarge” centripetally to fill the hematoma.
Large hematomas than can lead to compartment syndromes and ultrasound-guided drainage might be indicated.
- Indirect injuries
Indirect or intrinsic injuries are lesions that result from excessive simultaneously contraction and elongation of the muscle fibres,
causing their destruction.
They are the most frequent lesions of the athlete and commonly affect the myotendinous junction.
Muscle risk factors are predominance of type II fibres (fast-twitch fibres),
extension over two joints and previous intrinsic injuries.
The most affected muscles are: the rectus femoris,
medial gastrocnemius and the hamstrings.
US imaging is crucial in confirming the clinical diagnosis,
grade the lesion and exclude possible complications.
Different classifications exist,
but the classification from Peetrons and colleagues is one of the most widely accepted.
It has a prognostic importance and classifies lesions in 3 groups:
- Grade 0: lack of ultrasonographic abnormalities;
- Grade 1 (elongation injury): small tear (<5% of the muscle);
- Grade 2 (partial tear): larger tear (5-50% of muscle affected);
- Grade 3 (complete rupture): > 50% of muscle affected;
Regarding other classifications,
the British athletics system and the Munich consensus system (Fig.
6) are among the most used.

Fig. 6: Classification of acute muscle disorders and injuries according to Munich consensus.
References: Mueller-Wohlfahrt H-W et al. Terminology and classification of muscle injuries in sport: The Munich consensus statement Br J Sports Med 2013; 47:342–350.
Peetrons grade 1 – elongation injury
Ultrasound can be normal,
or depict areas of ill-defined increased echogenicity at the injury site (Fig.
7).
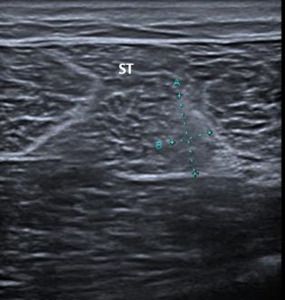
Fig. 7: Patient with a grade 1 Peetrons indirect injury at the semitendinous muscle. An ill-defined area increased echogenicity associated with loss of perimysial striation (between calipers) is identified at the middle third of the semitendinous muscle. No tear is identified. ST – semitendinous muscle.
Fibre disruption can be also be seen,
with loss of perimysial striation,
involving less than 5% of the muscle substance in transverse section (Fig.
8).

Fig. 8: Patient with a grade 1 Peetrons indirect injury at the vastus lateralis. An area of increased increased echogenicity in the distal third of the vastus laterais (V LT), in which a focal fiber disruption with hypoechoic fluid collection is identified (representing less than 5% of the muscle in the transverse section – outlined by calipers in a).
Dynamic study can be important in these cases to depict very small tears.
Despite their small size on transversal plane,
lesions can nevertheless span over a great longitudinal extent.
These lesions can have up to 10mm on cross-sectional diameter.
However,
there are some authors that consider any degree of fibre disruption as a grade 2 lesion.
Perifascial fluid can be seen,
sometimes with hyperechoic structure,
due to the presence of blood.
Peetrons grade 2 – Partial rupture
Lesions are considered grade 2 if they involve between 5 and 50% of the muscle in cross-sectional area.
US will demonstrate areas of fibre disruption,
with loss of perimysial striation (Fig.
9) and eventually an anechoic gap between the muscle fibres,
corresponding to hematoma (Fig.
10).
These lesions will happen mainly at the myotendinous or myofascial junction.

Fig. 9: Rugby player with a anterior thigh straing during competition. Despite the absence of hematoma, distortion of the perymysial architecture (area between calipers) is the sign of rupture involving the central tendon (arrowhead - Peetrons grade 2 muscle injury). This is a frequent presentation of ruptures involving the central tendon of this muscle. RF – Rectus femoris muscle.
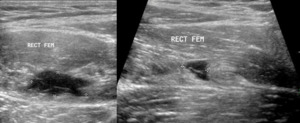
Fig. 10: Patient with a grade 2 Peetrons indirect injury at the rectus femoralis. An intramuscular hypoechoic fluid collection (hematoma) is seen , representing fibre rupture. In the transverse plane, less than 50% of the muscular cross-sectional area is injured.
Peetrons grade 3 – Complete rupture
These are complete muscle tears with retraction.
Usually they are clinically evident because the muscle belly forms a real mass and the gap between the retracted ends of the muscle can be palpated.
US shows subtotal or total muscle disruption,
with the torn ends retracted,
and an intramuscular hematoma.
Perifascial fluid may also be depicted.
If the torn fibres can be seen floating in a serohematic fluid it is called the "bell clapper sign” (Fig.
11).
There is hyperechogenicity of the surrounding fibers,
as well as hypervascularization.
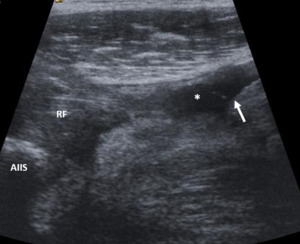
Fig. 11: Patient with a proximal rupture of the rectus femoralis. The bell-clapper sign is the mostrated by the rounded margin of the distal retracted muscle (arrow) floating in the surrounding hematoma (asterisk). RF – rectus femoralis proximal end; AIIS – anterior inferior iliac spine.
Despite this grading,
the most important to mention in the report and that will affect the clinical management of the athlete is the presence of muscule tear and hematoma,
which require longer sports interruption (4-6 weeks compared to 2 weeks without tear).
- The role of MRI
Ultrasound has shown equivalent accuracy to MRI in detecting muscle injury in the acute phase (< 48 hours).
However,
in grade 1 lesions without macroscopic rupture,
MRI has a greater sensibility,
perfectly depicting subtle areas of edema (Fig.
12).
Nonetheless,
for identifying very small tears US has a greater sensibility than MRI,
because of its superior spatial resolution.
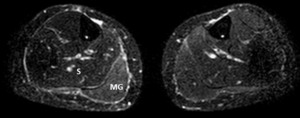
Fig. 12: Patient with a direct blow over the right calf during competition. The US findings were normal, with the muscles showing normal echogenicity and architecture. MRI done at the same day revealed mild diffuse increased signal on the medial gastrocnemius (STIR sequence), at the site of maximal pain, representing muscular edema. The right soleus and the contralateral medial gastrocnemius show normal signal, for comparison. MG – Medial Gastrocnemius; S – Soleus muscle.
- Follow-up and return to competition
US can also be used in the follow-up of injuries,
to demonstrate healing or eventual complications,
usually after 5-7 weeks.
It can also guide interventional procedures. MRI could be reserved for discrepant cases,
in which the clinical findings are not consistent with the sonographic changes or if the muscular injury does not heal in the expected time.
The return to competition is nowadays guided by clinical factors and the is a great overlap of recovery time between injuries of different grades.
Nevertheless,
imaging techniques might be relevant to demonstrate complete healing before the return.
They can also show fascial involvement or allow the identification of the exact muscles affected,
which may have different recovery times (the femoral biceps takes longer to heal than the semimembranous or the semitendinous).
- Apophysis avulsion injuries
In the skeletal immature athlete,
a powerful tensile force caused by muscle contraction will lead to injury of the weakest point of the muscle-tendon-bone unit,
which is the apophysis.
So,
when performing US in young athletes,
it’s very important to study the nearby apophysis.
When the apophysis avulsion is nondisplaced or the apophysis is not yet ossified,
the radiograph might be negative,
while ultrasound and MRI might reveal the lesion.
Widening of the hypoechoic physis between the apophysis and the bone or displacement of the apophysis are important sonographic signs of avulsion or instability (Fig.
13).
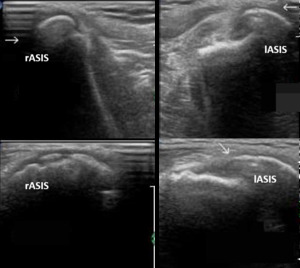
Fig. 13: 14 year old male sprinter who felt a sudden intense left anterior hip pain while accelerating during a competition. Apophysis lateraland inferior dislocation is seen (arrow in the lower right image) comparing with the contralateral site, representing avulsion fracture caused by the strong contraction of the Sartorius muscle. Note that both apophysis are already ossified at this stage and slight irregularity can be seen in the normal apophysis (c). Top images are made in the axial plane and the lower imagens on the sagital plane. rASIS – Right Anteriorsuperior Iliac Spine; lASIS – Left Anteriorsuperior Iliac Spine;
Apophysis avulsion injuries are common in the athletic children,
namely in: the ischial tuberosity (origin of the hamstrings); anterior superior (origin of the sartorius and tensor fascia lata muscle) and anterior inferior iliac spines (origin of the straight head of the rectus femoris); pubic symphysis (origin of the adductor brevis,
longus and the gracilis muscle).
- Delayed onset muscle soreness (DOMS)
DOMS might be seen 12-24 hours after unaccustomed exercise,
but might also be seen in elite athletes,
typically during pre-season.
It represents reversible microstructural damage to the muscle and inflammatory reaction.
These patients have increased serum creatine kinase levels.
US might be normal or reveal swollen hyperechoic muscles in different compartments (Fig.
14).
There is a typical resolution of symptoms in 4-5 days.
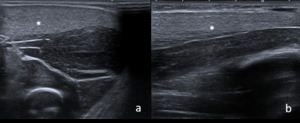
Fig. 14: Young physician submitted to an extreme physical exercise after a prolonged sports interruption and developed a DOMS syndrome. US reveales a diffusely thickened and hyperechoic muscle (asterisks in transverse and longitudinal planes – a and b, respectively). Compare to the normal underneath muscle. Clinical resolution was noticed after 1 week of resting.
DIFFERENTIAL DIAGNOSIS
Sometimes the hematoma may simulate tumors,
particularly sarcomas.
In these cases,
the age of the patient (tumors can be found at any age but intramuscular tumors are more frequent after 40 years) clinical story,
the vascularization study (Color Doppler and Power Doppler) and the evolution is very important.
If any doubt,
short-term follow-up exams (approximately after 2 weeks) or MRI should be done (Fig.
15).
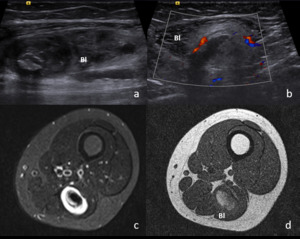
Fig. 15: 12 year old patient that palpated mass in the posterior thigh. No history of trauma was recalled. An heterogenous mass in seen in within the biceps long head in US(a). Transverse sonogram (b) demonstrated peripheral hypervascular hyperechoic structure surrounding a fluid collection (box in b. The possible diagnosis were, at this time, muscular rupture with hematoma and tumor so MRI was done in the following day. STIR (c) and T1-wheighted (d) images demonstrate the intramuscular location of the mass with peripheral increased signal on STIR (corresponding to the hyperchoic area seen in b) and fluid centre containing blood (mild hypersignal in d) allowing the diagnosis of muscular rupture. US follow-up demonstrated resolution of the findings at 4 weeks. Bl – Femoral biceps long head.
Deep venous thrombosis is probably the leading differential diagnosis for leg pain and swelling,
which can mimic muscle rupture. US,
particularly US Doppler,
is the first-line technique to search for this diagnosis.
Moreover,
deep venous thrombosis can also be a complication of muscle rupture.
A ruptured Baker cyst is also an important differential diagnosis since it can present clinically with calf pain and swelling.
US might reveal the correct diagnosis (video in image 16).
Fig. 16: A 48 years-old female complained of sudden onset intense calf pain and tenderness after running. US reveals large cyst collection (asterisk) arising from the popliteal fossa (cyst neck), between the tendon of the semimembranosus and the tendon of the medial gastrocnemius head. The fundus of the cyst continues with fluid that spreads over the calf. SM - semimembranous muscle; MHG - medial head of gastrocnemius.

. Increased thickness of the medial gastrocnemius is seen, showing an hyperechoic structure than can also be seen in the most superficial fibres of the soleus muscle, consistent with contusion (c and d in transversal and longitudinal sections, respectively). Note that the increased echo attenuation caused by the thickned gastrocnemius does not allow a proper evaluation of the soleus muscle, despite the low position of the focus (transverse sonogram in c). No signs of tear are identified. MG – Medial gastrocnemius; S – Soleus muscle.")
 is identified at the middle third of the semitendinous muscle. No tear is identified. ST – semitendinous muscle.")
, in which a focal fiber disruption with hypoechoic fluid collection is identified (representing less than 5% of the muscle in the transverse section – outlined by calipers in a).")
 is the sign of rupture involving the central tendon (arrowhead - Peetrons grade 2 muscle injury). This is a frequent presentation of ruptures involving the central tendon of this muscle. RF – Rectus femoris muscle.")
 is seen , representing fibre rupture. In the transverse plane, less than 50% of the muscular cross-sectional area is injured.")
 floating in the surrounding hematoma (asterisk). RF – rectus femoralis proximal end; AIIS – anterior inferior iliac spine.")
, at the site of maximal pain, representing muscular edema. The right soleus and the contralateral medial gastrocnemius show normal signal, for comparison. MG – Medial Gastrocnemius; S – Soleus muscle.")
 comparing with the contralateral site, representing avulsion fracture caused by the strong contraction of the Sartorius muscle. Note that both apophysis are already ossified at this stage and slight irregularity can be seen in the normal apophysis (c). Top images are made in the axial plane and the lower imagens on the sagital plane. rASIS – Right Anteriorsuperior Iliac Spine; lASIS – Left Anteriorsuperior Iliac Spine;")
. Compare to the normal underneath muscle. Clinical resolution was noticed after 1 week of resting.")
. Transverse sonogram (b) demonstrated peripheral hypervascular hyperechoic structure surrounding a fluid collection (box in b. The possible diagnosis were, at this time, muscular rupture with hematoma and tumor so MRI was done in the following day. STIR (c) and T1-wheighted (d) images demonstrate the intramuscular location of the mass with peripheral increased signal on STIR (corresponding to the hyperchoic area seen in b) and fluid centre containing blood (mild hypersignal in d) allowing the diagnosis of muscular rupture. US follow-up demonstrated resolution of the findings at 4 weeks. Bl – Femoral biceps long head.")