IDIOPATHIC INTRACRANIAL HYPERTENSION
Idiopathic intracranial hypertension (IIH) is characterized by raised ICP of unknown cause.
It is rare but important disease associated with significant morbidity,
including permanent vissual loss in up to 25% of cases.
Incidence of IIH is steadily increasing (1-2 per 100.000 population).
Females are more affected than males (tipically affecting young women of childbearing age).
Children as young as 4 months can be affected with equal sex distribution.
IIH has been associated with conditions related to increased intra-abdominal,
visceral fat and elevated body mass index (BMI),
such as elevated leves of asipose tissue-derived retinol binding protein,
polycystic ovarian disease in womeen and androgen deficiency in men.
BMI has a linear relationship with CSF pressure.
Pathophysiology
Raised ICP is a uniform characteristic,
but underlying pathogenesis of IIH is uncertain.
Changes of the volume of blood,
CSF and brain tissue influencen ICP.
IIH likely represents a disorder of CSF regulation,
potentially through CSF hypersecretion or reduced drainage.
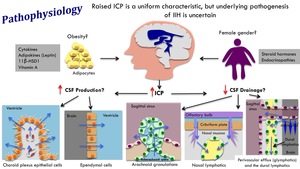
Fig. 2: Pathophysiology of idiopathic intracranial hypertension
Increased CSF production:
- Choroid plexus is the primary site of CSF production.
Rest comming from ependyma and blood brain barrier.
- In choroid plexus,
CSF production is governed by ion transporters located on epithelial cells.
Net movement of ions across these cells results in movement of water and secretion of CSF.
- Ventricular size is NOT altered in IIH,
making CSF hypersecretion unlikely.
- Disregulation of fluid transport in IIH is important.
Aquaporin 1 channels are predominantely in the choroid plexus,
can be upregulated by retinoids and glucocorticoids,
and affected by medications used to treat IIH.
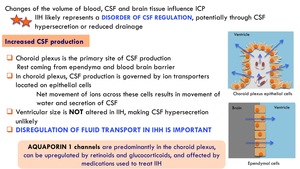
Fig. 3: Pathophysiology. Increased CSF production
Reduced CSF drainage:
CSF drains: 1) from the subarachnoid space into the superior sagittal sinus,
2) through cranial nerves and cribiform plate into lymphatics
Newly named "glymphatic pathway" suggests an exchange in fluid between the CSF in the subarachnoid space and the interstitial fluid in the brain along paravascular routes.
Reduction in CSF absorption by arachnoid granulations may be attributed to increase in CSF outflow resistance or reduction in pressure gradient between the subarachnoid space and the superior sagittal sinus.
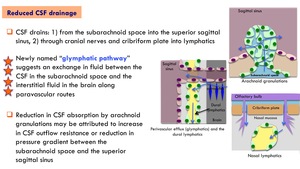
Fig. 4: Pathophysiology. Reduced CSF drainage
Clinical features
- Visual loss papilledema. Majority of patients with papilledema suffer visual loss.
- Headache. Most common presenting symptom.
Daily,
bilateral,
frontal or retroocular.
Associated with back,
neck and radicular pain.
- Pulsatile tinitus. Uni or bilateral.
- Diplopia. Affects 1/3 to 2/3 of patients with IIH at presentation.
It can be binocular and horizontal (abducens nerve palsy),
and resolves with normalization of ICP.
Monocular diploplia is due to severe papilledema.
- Transients visual obscurations (TVO). Related to postural changes or straining.
NO longer than a minute (one-both eyes).
Due to disc edema causing transient ischemia at the optic nerve head.
- Mood disturbance
- Impairments in memory and concentration
Diagnostic criteria

Fig. 5: Diagnostic criteria
Comorbidities
Polycystic ovarian syndrome (PCOS) is a chronic endocrine condition characterized by menstrual irregularities,
ovarian dysfunction,
hyperandrogenis,
and hirsutism.
Prevalence of PCOS in women with IIH is reported to be as high as 39-57% (7-18% in general population).
Similar to IIH,
PCOS is a disorder of women of childbearing age,
associated with obesity,
high serum leptin levels and low-grade inflammation.
Metabolic syndrome is a collection of risk factors including abdominal obesity,
insulin resistance,
circulating hypertriglyceridemia and hypertension that combined increased the risk of developing type II diabetes mellitus,
cardiovascular and cerebrovascular disease.
Obese phenotype of patients with IIH suggests that these patients may be at risk of metabolic syndrome.
Treatment
Acetazolamide is considered the first-lines medication for the treatment of IIH.
It inhibits carbonic anhydrase in the choroid plexus to decreased CSF production,
and thereby,
reduces ICP.
The idiopathic intracranial hypertension treatment trial (IIHTT) showed statistically significant effects of acetazolamide to:
- Improve visual field function
- Decrease papilledema grade
- Improve quality of life measures
- Decrease CSF pressure
Reducing ICP has led to resolution of stenosis in some patients,
suggesting that stenosis are a result of raised ICP externally deforming the venous sinuses,
and not a primarily cause.
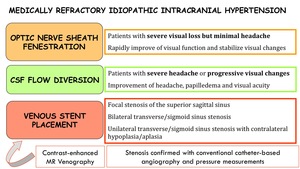
Fig. 6: Medically refractory idiopathic intracranial hypertension
SPONTANEOUS INTRACRANIAL HYPOTENSION
Incidence of SIH is 5 per 100.000 patients and year.
Affects women twice as frequently as men (female/male ratio of 3:2).
Typically presents in the fourth or fifth decade of life,
but children and elderly can also be affected.
For patients with SIH,
underlying CSF leak should be looked in the spine and NOT at the skull base.
Pathophysiology
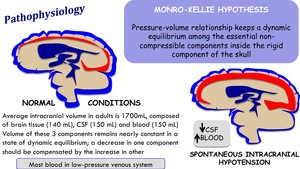
Fig. 7: Pathophysiology of spontaneous intracranial hypotension
Spontaneous CSF leakage has been reported mostly as ocurring at the cervicothoracic and thoracolumbar junction of the spine.
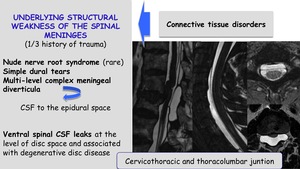
Fig. 8: Pathophysiology. Underlying structural weakness of the spinal meninges
Clinical features
Classic symptom: positional headache that worsens in the upright position + neck stiffness and subjective hearing symptoms
Symtoms secondary to nerve traction and mass effect on intracranial structures:
- Cranial nerve dysfunction
- Visual disturbance
- Tinnitus,
diziness
- Neck pain and/or radiculopathy
- Dementia
- Altered consciousness
Diagnosis
Diagnostic criteria proposed by Schievink,
2008 (modified 2011):
Orthostatic headache
The presence or at least one of the following:
- Low opening pressure (≤60 mmH2O)
- Sustained improvement of symptoms after epidural blood patching
- Demonstration of an active spinal CSF leak
- Cranial MRI changes of intracranial hypotension (eg,
brain sagging or pachymeningeal enhancement)
No recent history of dural puncture
Not attributable to another disease
Treatment
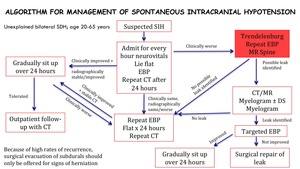
Fig. 9: Algorithm for management of spontaneous intracranial hypotension








