ECR 2019 / C-0185

Neurooncology pending battles: is it possible to differentiate true progression from pseudoprogression?
Congress:
ECR 2019
Poster Number:
C-0185
Type:
Educational Exhibit
Keywords:
Neoplasia, Multidisciplinary cancer care, Radiation effects, Diagnostic procedure, MR-Diffusion/Perfusion, MR, Neuroradiology brain
Authors:
A. Hilario Barrio, P. Martín Medina, E. Salvador, G. Ayala, L. Koren, A. Martinez de Aragon, F. Ballenilla, J. M. Millan, A. Ramos Gonzalez; Madrid/ES
DOI:
10.26044/ecr2019/C-0185

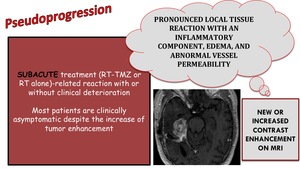
Fig. 3:
Subacute treatment-related changes that appears as new or increased contrast...

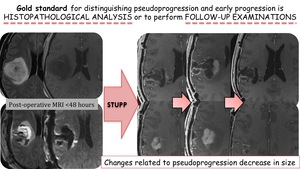
Fig. 4:
Gold standard for distinguishing pseudoprogression and early progression

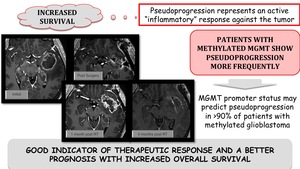
Fig. 5:
Increased overall survival related to pseudoprogression

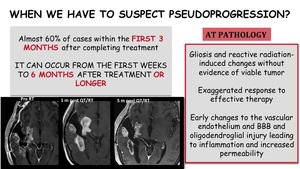
Fig. 6:
When we have to suspect pseudoprogression?

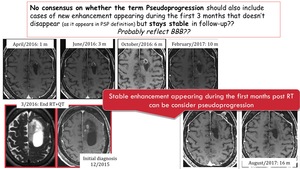
Fig. 7:
No consensus whether the term PsP should also include a new enhancement...

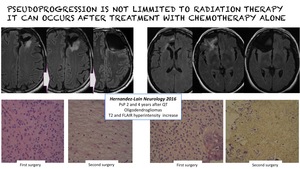
Fig. 8:
Pseudoprogression can occur after treatment with chemotherapy alone

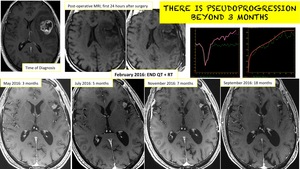
Fig. 9:
Pseudoprogression beyond 3 months