The parotid gland is the largest of the salivary glands and secretes saliva via the parotid duct into the oral cavity to facilitate mastication and swallowing.
It is located in the parotid space.
PAROTID GLAND ANATOMY
- The parotid gland is located in the retromandibular fossa,
anterior to the ear and sternocleidomastoid muscle.
Parts of the superficial lobe cover the ramus of the mandible and the posterior part of the masseter muscle.
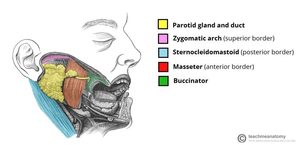
Fig. 1
References: teachmeanatomy
- The border between the superficial and deep parotid lobes is created by a plane in which the facial nerve and its branches are located, as does the external carotid artery (ECA) and retromandibular vein.
The ECA forms its two terminal branches within the parotid gland: maxillary and superficial temporal artery.
There is moderate fatty infiltration or fatty replacement of the parotid glands with age.
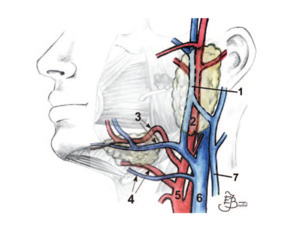
Fig. 2: Drawing shows the major blood vessels in the area of the salivary glands.
1 retromandibular vein, 2 external carotid artery, 3 facial artery and vein, 4 lingual artery and vein, 5 external carotid artery, 6 internal jugular vein, 7 external jugular vein.
References: Bialek E, Jakubowski W, Zajkowski P, Szopinsk K, Osmolski . US of the Major Salivary Glands: Anatomy and Spatial Relationships, Pathologic Conditions, and Pitfalls. RadioGraphics 2006; 26:745–763.
- There is a fibrous capsule surrounding the gland,
formed by the split layers of the investing layer of the deep cervical fascia.
Posteriorly this fascia condenses forming the stylomandibular ligament. The inferior projection of the parotid is often referred to as the "tail" which overlies the angle of the mandible.
Anteriorly there is often an accessory parotid gland which may be separate to the main gland.
The accessory parotid gland may also be the site of salivary gland tumors,
benign or malignant.
The main excretory duct ( Stenon duct) lies on the masseter muscle,
about 1 cm below the zygomatic arch, then crosses the buccal muscle and has its orifice in the parotid papilla at the level of the upper second molar.
The length of the Stenon duct usually varies between 3 and 5 cm.
A nondilated duct is usually not visible during US examination.
In the parenchyma of the parotid gland,
lymph nodes may be found.
They are localized mainly in the area of the upper and lower poles of the gland.
Normal intraparotid lymph nodes may be oval or have a longitudinal shape.
IMAGING TECHNIQUES FOR THE EVALUATION OF PAROTID GLAND
1.
ULTRASOUND
- Ultrasound is often the first diagnostic procedure to evaluate morphological and structural changes of the parotid gland; for small (<3 cm) and superficial lesions,
ultrasound and cytology are often sufficient for a definitive diagnosis.
- It is a harmless,
simple and cheap image method.
Allows to differentiate the injuries solid of the cystic,
detect the calcifications,
study the adenopathies,
assess the vascularization of the lesions with the color Doppler technique,
and also serves as a guide for FNA (fine needle aspiration).
- It is carried out with 7-12 Mhz high-frequency linear transducers,
applying them at least in two perpendicular planes.
- The normal echogenicity of the parotid gland is generally homogeneous and varies from very bright and markedly hyperechoic to only slightly hyperechoic in comparison to adjacent muscles.
The echogenicity depends on the amount of intraglandular fatty tissue.
- Stenon's duct is usually only visible if it is dilated.
- The facial nerve is not visible by US,
therefore,
the retromandibular vein (located above of the facial nerve trunk),
it is used as a reference point that separates the lobes superficial and deep.
- The deep parotid lobe can be visualized only partially at US.
Some areas of glandular parenchyma and possible lesions may be hidden in the acoustic shadow behind the mandibular ramus.
- Intraparotid lymph nodes are normally seen (unlike the submandibular gland).
- Limitations of ultrasound are:
- difficulty visualizing deep lesions: the deep lobe is not able to be assessed as it is protected by the mandibular ramus
- difficulty visualizing deep extension
2.
SIMPLE RADIOGRAPHY
Indications:
1.
Useful for the study of radiopaque lithiasis.
2.
It also allows to exclude the mandibular bone pathology that resembles glandular disease.
3.
COMPUTED TOMOGRAPHY (CT)
Indications:
1.
Assess the glandular parenchyma and adjacent soft tissues.
2.
See if there is a compromise of the adjacent bone structures (base of the skull,
jaw).
3.Distinguish the presence of non-palpable lymph nodes.
4.Evidence lithiasis.
5.Evaluate the parapharyngeal and retromandibular spaces.
The parotid gland is seen like a structure hypodense (15-25 UH) with respect to muscles and higher density than fat.
The Stenon's duct can sometimes be visualized even if it is not dilated.
The external carotid artery and retromandibular vein show greater attenuation and are located behind the jaw.
4.
MAGNETIC RESONANCE (MR)
Same indications as CT,
but it has a higher resolution of the soft parts:
1.
Differentiation of superficial tumor of a deep one.
2.
Better delimitation of Tumor lesions.
3.
To evaluate nerve structures.
Study protocol: axial T1 SE,
axial T2 FSE FATSAT,
coronal T2 FATSAT,
sialo-RM T2 sagittal.
It is completed with other T1 sequences with contrast if there is a tumor.
The normal parotid shows intermediate or high signal in T1 due to its content fatty,
and intermediate or low in T2.
5.
SIALOGRAPHY
Currently little used.
It is done by injecting an iodinated radiopaque contrast medium retrogradely to through the Stenon conduit.
This procedure must always be bilateral.
Ideally, the medium must be water-soluble since oleaginous,
if extravasated,
can produce granulomas.
-Indications:
1.
Evaluate the canal system: identifying stones,
mucous plugs,
stenosis.
2.Estudy of chronic diseases: recurrent chronic sialadenitis gives an image in "rosary beads" (dilatations of intraglandular canaliculi with formation of stenosis and dilatations that vary in size and location) and in benign lymphoepithelial sialoadenopathy,
multiple small cavities are observed uniforms,
distributed diffusely.
3.Cysts
4.Fistulas
-Contraindications: acute inflammation and iodine allergy.


