Of the 33 patients (42 MR exams),
3 patients (3 MR exams) were excluded due to biopsy proved mucinous tumors and 2 patients (2 MR exams) were excluded due to nondiagnostic image quality (hip replacement).
Moreover,
7 MR exams with missed pathology (surgery performed after neoadjuvant treatment) were excluded.
A total of 24 patients (29 MR scans) met the inclusion criteria and constituted the final study population (57 ± 12 years,
mean age ± SD).
Of the 29 MR scans,
18 (62%) were performed at the primary staging and 11 (38%) at the end of neoadjuvant treatment (8 weeks after completion of neoadjuvant treatment).
At baseline,
all 18 patients had biopsy-proven rectal tumors.
Of those 11 (38%) patients for whom imaging was performed at the end of neoadjuvant treatment,
6 (21%) showed pathologic complete response and 5 (17%) had residual tumor at pathology.
In 2 (0.7%) of the study scans,
both performed at the end of neoadjuvant treatment,
severe artefacts were present and thus were excluded leaving a total of 9 (31%) restaging MR examinations for further qualitative and quantitative evaluation.
More specifically,
those artefacts were caused by air induced susceptibility effects resulting in severe distortions and “ghosting artifacts”,
which were noted to be more severe for b2000.
Tumor detectability on b1000 vs.
b2000 DWI
On the 18 baseline MR exams,
both readers correctly identified (i.e.
score of ≥1) the presence of tumor in all 18 cases,
both on b1000 DWI as well as on b2000 DWI.
On the 9 restaging scans performed after completion of chemoradiotherapy (CRT),
both readers correctly identified the presence (i.e.
score ≥1) or absence (score 0) of residual tumor on both b-values,
except in one residual tumor case in which both readers assigned a score of 0 on b1000 DWI,
but correctly detected the residual tumor on the b2000 images,
albeit with a low tumor conspicuity score of 1 for both readers,
indicating moderate demarcation.
Tumor conspicuity on b1000 vs b2000 DWI – qualitative analysis
Results of the qualitative analysis are shown in Table 3.
For the patients in whom a tumor lesion was detected on DWI,
mean overall conspicuity scores were higher for b2000 compared to the b1000 images (3.57 versus 2.85 for Reader 1,
p=0.001; 3.0 versus 2.45 for Reader 2,
p=0.002).
Representative imaging examples are provided in Figures 3 (baseline MRI) and 4 (after CRT).
Interobserver agreement was good for both b-values (k = 0.71 for b=1000 s/mm2 ,
k = 0.65 for b=2000 s/mm2 ).
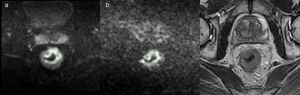
Fig. 3: b=1000 s/mm2 diffusion weighted image (a), b=2000 s/mm2 diffusion weighted image (b) and
T2-weighted image (c) selected from a 68-year-old man MR staging with biopsy proved rectal
adenocarcinoma. In b=2000 s/mm2 image, the improved background suppression allows an easier tumor
delineation.
References: Department of Radiology and Bioimaging, "G. D'Annuzio" University, Chieti-Pescara, "Ss. Annunziata" - Chieti - Chieti/IT
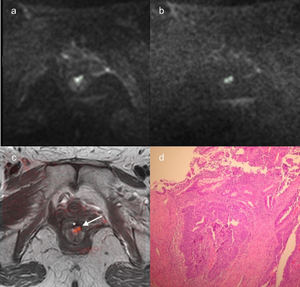
Fig. 4: b=1000 s/mm2 diffusion weighted image (a), b=2000 s/mm2 diffusion weighted image (b) and
fusion T2-weighted images and b=2000 s/mm2 diffusion weighted image (c) selected from a 65-year-old
woman MR scan performed at the end of neoadjuvant treatment for rectal cancer. Patient was a noncomplete responder. The two small residual tumor foci (white arrow in c) near the radiation therapy-induced
fibrosis (*) were clearly depicted when using b=2000 s/mm2 thanks to the better background suppression
and they were pathologically confirmed (d).
References: Department of Radiology and Bioimaging, "G. D'Annuzio" University, Chieti-Pescara, "Ss. Annunziata" - Chieti - Chieti/IT
Tumor conspicuity on b1000 and b2000 DWI – quantitative analysis
In the tissue surrounding the tumor,
the mean signal intensity was significantly lower when using b2000 (p<0.05).
On the contrary,
the mean signal intensity of the tumor was significantly higher in b1000 (p<0.05).
When considering the whole tumor,
the variance,
10th percentiles and 90th percentiles were significantly lower in b2000 (p<0.05),
meaning that signal intensity was more homogenous (variance) and less affected by outliers (10th percentiles and 90th percentiles) compared to b1000.
In the same way,
variance and 90th percentiles were significantly lower in the healty surrounding tissues (p<0.05) when using b2000 (p<0.05).
Regarding 10th percentiles,
their mean value was lower in b2000 but there were no statistical differences with 90th percentiles.
The inter-observer agreement for the signal intensity in the tumor bed improved from b1000 to b2000 (ICC = 0.60 and 0.79,
respectively).
(Fig.
5)

Fig. 5: Box plots comparing the mean signal intensity, variance, 10th percentile and 90th
percentile of b=1000 (s/mm2
) and b=2000 (s/mm2
) considering the whole tumor delineation and the
tissue surrounding the tumor.
References: Department of Radiology and Bioimaging, "G. D'Annuzio" University, Chieti-Pescara, "Ss. Annunziata" - Chieti - Chieti/IT
Tumor detectability
On the pre-treatment MRIs all tumors were correctly identified with both b1000 and b2000 DWI by both readers.
On the restaging MRIs,
in one case the tumor was detected only on b2000 DWI (albeit with low conspicuity) and could not be identified on routine b1000 DWI.
Interobserver agreement was comparably good for both b-values.
The conspicuity quantitative analysis of the whole tumor and the tissues surrounding the tumor showed significant differences in terms of mean signal intensity,
variance,
10th - 90th percentile between the two b-values,
in favour of the b2000 images,
thus validating the results of conspicuity qualitative assessment.
The reduced signal intensity in the tumor surrounding tissues obtained with b=2000 images resulted in a higher conspicuity.
Due to a better background suppression,
the tumor was more prominently visible,
therefore facilitating the delineation of tumor itself.
Higher conspicuity was further confirmed by the excellent ICC (0.79 vs 0.60 for the b1000 images) and by higher qualitative lesion conspicuity scores reported by both readers.
Furthermore,
the variance,
10th and 90th percentiles of the tumor and of the adjacent tissues,
were lower in b2000,
suggesting that images were less affected by noise and outliers compared to b1000.
A potential downside of the b2000 images,
was that – in addition to the reduced signal in the tumor surrounding tissues – the mean signal intensity in the tumor itself was also lower compared to b1000.
This was an expected finding,
since the increase of the diffusion weighting is responsible for a reduction in the signal-to-noise ratio,
with a consequent overall decrease in mean signal intensity.
Moreover,
the overall reduced signal also results in less anatomical detail,
which may lead to the loss of potentially valuable information and could pose a potential diagnostic challenge.
However,
b2000 images are usually acquired with a set of lower b values,
thus limiting the weight of the above mentioned disadvantages.
Moreover,
based on our results it appears that the beneficial effect of the improved lesion-to-background ratio outweighs the potential downsides of a higher b value,
particularly for the less experienced reader.
In other words,
for readers with less experience,
the complete suppression of all background signal can make the detection of a bright tumor lesion more straightforward and therefore easier.
A final downside of increasing the diffusion-weighting is that images will typically become more susceptible to distortions,
"ghosting artifacts" and increased spatial blurring due to eddy currents.
In two of the study scans,
these artefacts were so severe that the scans had to be excluded from the analysis.

, b=2000 s/mm2 diffusion weighted image (b) and
T2-weighted image (c) selected from a 68-year-old man MR staging with biopsy proved rectal
adenocarcinoma. In b=2000 s/mm2 image, the improved background suppression allows an easier tumor
delineation. References: Department of Radiology and Bioimaging, "G. D'Annuzio" University, Chieti-Pescara, "Ss. Annunziata" - Chieti - Chieti/IT")
, b=2000 s/mm2 diffusion weighted image (b) and
fusion T2-weighted images and b=2000 s/mm2 diffusion weighted image (c) selected from a 65-year-old
woman MR scan performed at the end of neoadjuvant treatment for rectal cancer. Patient was a noncomplete responder. The two small residual tumor foci (white arrow in c) near the radiation therapy-induced
fibrosis (*) were clearly depicted when using b=2000 s/mm2 thanks to the better background suppression
and they were pathologically confirmed (d). References: Department of Radiology and Bioimaging, "G. D'Annuzio" University, Chieti-Pescara, "Ss. Annunziata" - Chieti - Chieti/IT")
 and b=2000 (s/mm2
) considering the whole tumor delineation and the
tissue surrounding the tumor.
References: Department of Radiology and Bioimaging, "G. D'Annuzio" University, Chieti-Pescara, "Ss. Annunziata" - Chieti - Chieti/IT")